Introduction
Intensive Care Units (ICUs) are spaces created to care for patients with and acute chronic diseases that require specialized assistance; therefore, ICUs are usually closed units where family members are separated from the patient at admission and are moved to the background, in order to focus the therapeutic efforts on the patient. However, hospitalization in an Intensive Care Unit not only affects the patient but also their family members, who present needs that should be met1.
If not solved, the family members' needs increase the uncertainty level, which causes in them countless problems, both of a physical and of mental and social natures. It is important to note that the family is an integral component of Nursing assistance as a care subject, reason why the professionals are required to apply interventions that allow modulating the uncertainty generated in the relatives, in addition to being a constitutional right2-4.
It is also relevant to state that the conventional care offered to family members by Nursing professionals is solely focused on making them sign the different consent forms at admission and, subsequently, on communicating with them to report if the patient has any type of diagnostic test scheduled that requires their presence.
The uncertainty generated in the family members at ICU admission is documented5,6 and middle-range theories such as Merle Mishel's instruct the professionals based on disciplinary knowledge about the measures to be adopted to care for the family member during this period3,7; it is because of the theory that the source of the problem can be understood and, in the same way, how to modulate it.
Given the aforementioned, the objective of the current study was to assess the effect of an educational Nursing intervention compared to conventional care on uncertainty in family members of patients hospitalized in an ICU.
Uncertainty of family members in an ICU
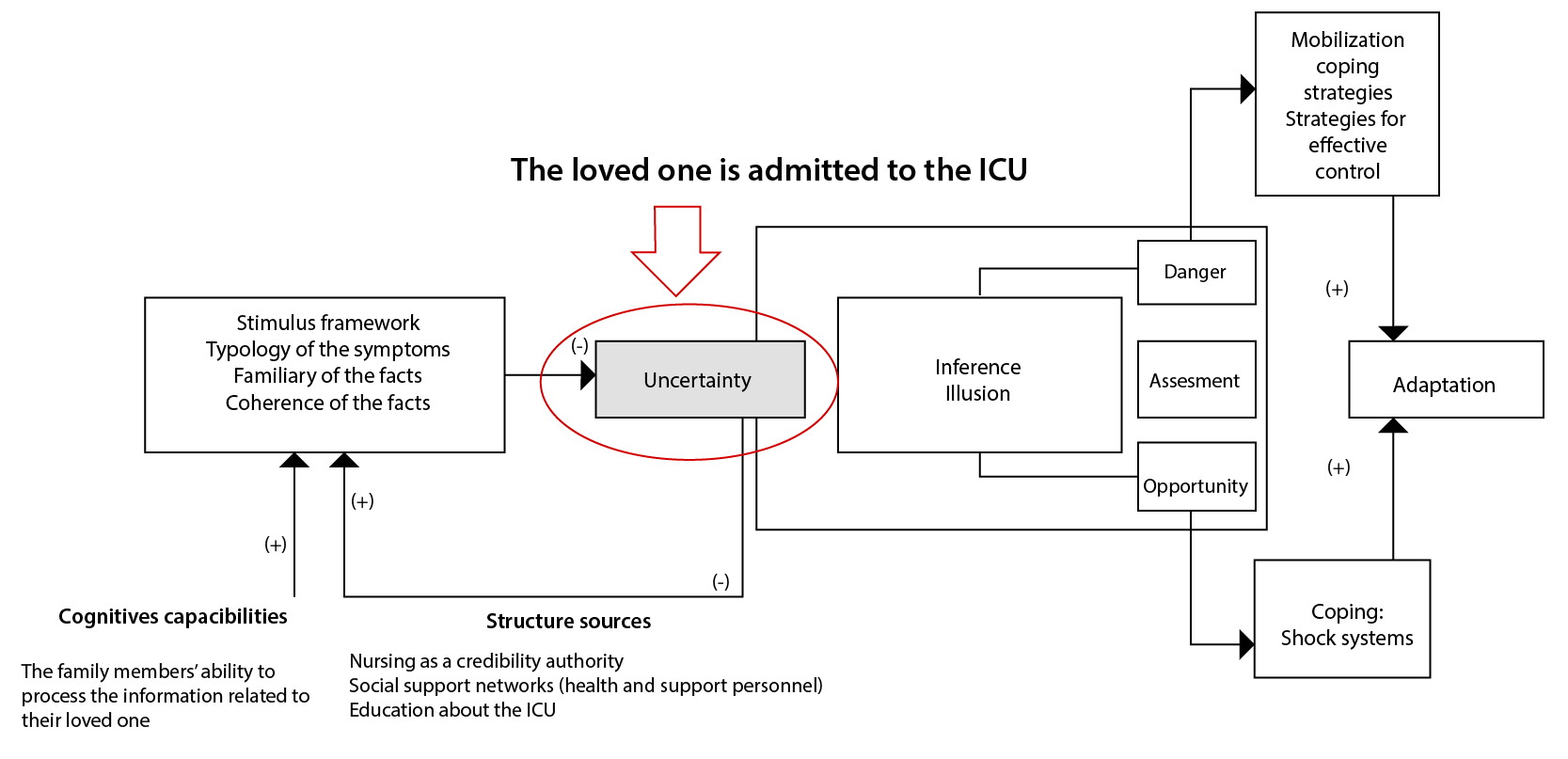
Uncertainty has its onset when the loved one is admitted to the ICU; due to the number of unexpected events, family members become incapable of attributing clear meanings to the situation3.
Likewise, among the concepts proposed by Mishel in her theory, the structure sources represent the existing resources to assist the person in interpreting what is happening8, which is comprised by:
- Credible authority: It is the degree of trust deposited by the person on the health personnel caring for them, which are Nursing professionals in this case, for being the health staff sharing the most time with the patient when compared to the other professionals9,10.
- Social support: The social support received exerts an influence on the uncertainty levels when it helps people interpret the meaning of the facts. Nursing professionals understand the concept of uncertainty and the effects it causes on family members; in addition, they apply suitable interventions so that the relatives can modulate it.
- Education: It reduces the uncertainty because, by having a knowledge base, it is possible to attribute meaning to the fact and to better understand it. It is characterized as with the objective of providing tools to the family members so that they make decisions based on the information offered about the treatment and the subsequent interventions and, thus, being able to include education about any aspects unknown by the family members about the ICU operation, components and health/support personnel, in addition to the care plan for the loved one. It is a prerequisite to elaborate clear meanings about the current event.
In relation to the family members' cognitive capabilities, they can vary according to each person; uncertainty has its onset when the loved one is admitted to the ICU; due to the number of unexpected events, family members become incapable of attributing clear meanings to the situation3. See Figure 1.
Materials and methods
Design: Experimental study with four Solomon groups: two experimental and two control, with random allocation.
Participants: The population consisted of the adult family members of patients hospitalized for the first time in the ICU for adults of a health institution from the city of Neiva, Colombia, during the 2020-2021 period.
Inclusion criteria: Adult family members of patients hospitalized for the first time in an ICU. Exclusion criteria: Adult family members of ICU-admitted patients that were not located or were not in due physical and mental conditions to answer during data collection.
Sample size: The sample was comprised by 132 family members; each group consisted of 33 relatives11. Allocation to the groups was defined in a simple random way, taking the following scheme into account (see Table 1 ).
Table 1. Solomon group experimental design scheme
X
Table 1. Solomon group experimental design scheme
| # |
Group |
Baseline assessment |
Intervention |
Final assessment |
| 1 |
Experimental 1 |
x |
x |
x |
| 2 |
Experimental 2 |
|
x |
x |
| 3 |
Control 1 |
x |
|
x |
| 4 |
Control 2 |
|
|
x |
Measurement variables: Disease uncertainty was assessed with Merle Mishel's Uncertainty in Illness scale, family member form (PPUS-FM), which has 31 items with a Cronbach's alpha of 0.81. This scale classifies the uncertainty level according to its final score, as follows: low UL with <61 points, fair UL with 61-89 points; and high UL with >89 points9. In addition, a sociodemographic data form was also included.
Randomization: The group allocation for the family members that met the inclusion criteria and gave the consent to participate in signing was performed in a simple random way, with a list of random numbers in Excel.
Procedure:The control groups were offered the conventional intervention, which consists in the interventions performed by the Nursing personnel to serve the family members of the individuals hospitalized in the ICU for adults. These care measures are focused on making the family member sign informed consent forms at the patient's admission and, subsequently, communicating with them to report if the patient has some type of diagnostic test scheduled that requires their presence.
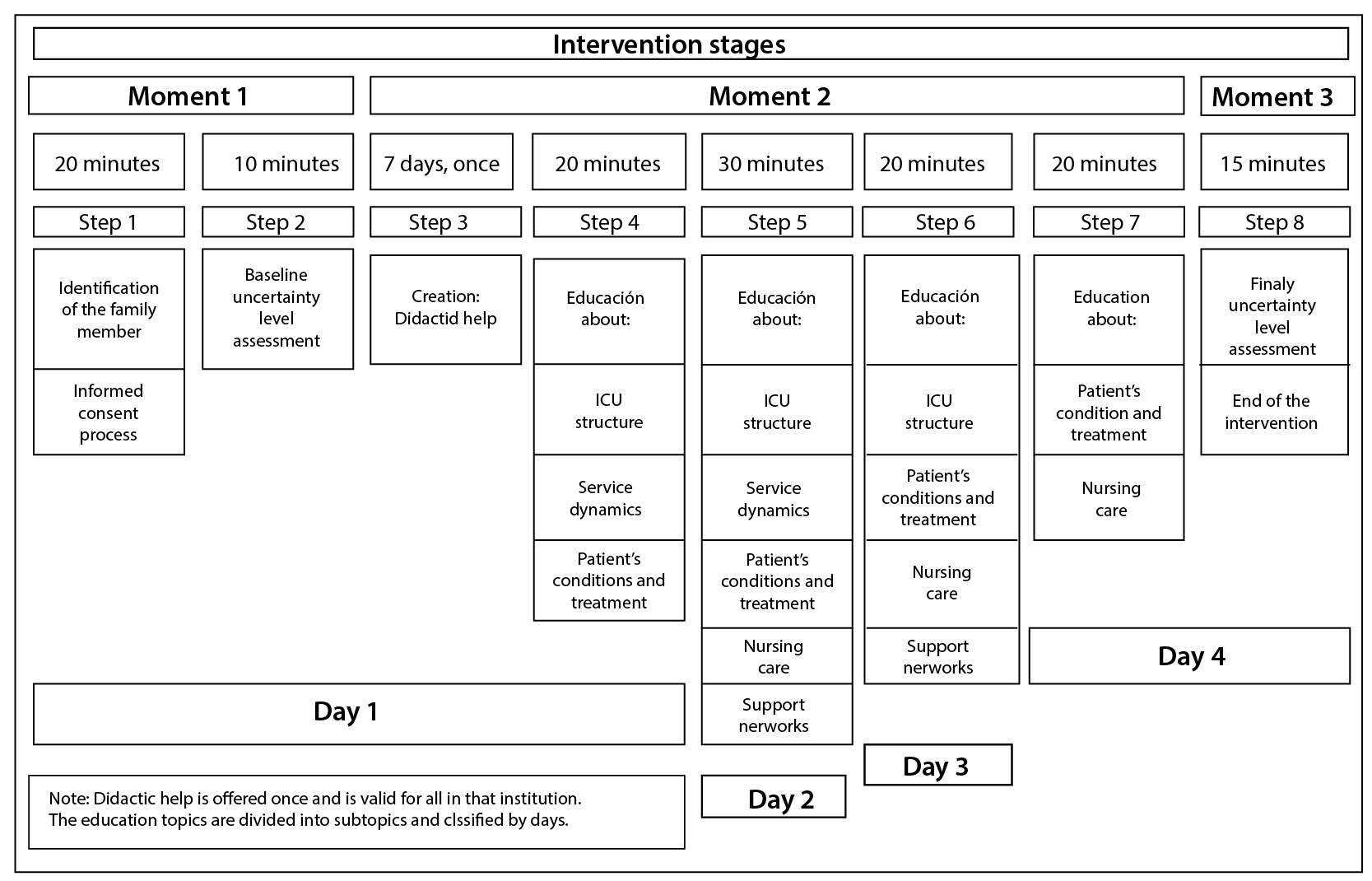
The Intervention Group was offered the educational Nursing intervention called “Acompañándote en la UCI” (“Being with you in the ICU”), which was prepared taking into account the concepts of cognitive capabilities and structure sources from Merle Mishel's Uncertainty in Illness Theory and Robin Whittemore's guidelines for the systematic development of Nursing interventions12. The Nursing intervention for relatives of patients hospitalized in the ICU is applied for four days and instructs on the following: ICU structure; service dynamics; patient's conditions and treatment; support networks; and Nursing care (see Figure 2). To ensure reliability of the intervention, an operations manual was prepared that explains in detail each moment and contains a checklist to ensure that the intervention is applied.
Data analysis: During the data analysis, an Excel document was generated in Google Forms, which was subjected to verification and debugging of incorrect and missing data; subsequently, the Statistical Package for Social Science, SPSS® (version 26) was used, under license by Universidad de La Sabana. The database was stored in Mendeley Data1713. Normality was verified with the Shapiro-Wilk test. The result indicated that the measurements in the groups do not correspond to normal distribution. The analysis of the data obtained was performed through two approaches:
- An intra-group approach that evaluated changes in the uncertainty levels
- An inter-group approach that compared changes in the uncertainty levels across the groups.
The analysis of the results in the intra-group analysis resorted to the Wilcoxon test for the experimental and control groups. In addition, the Mann-Whitney U test was performed in the analysis of the inter-group results and, finally, the ANOVA test was applied in Experimental Group 1 and Control Group 1, in order to verify the need to collect a baseline measure or not.
Ethical considerations
The research observed the ethical principles of research as per Resolution No. 8430 of 199314, as minimal risk. The international and national guidelines for research in health were respected. It was approved by the Research and Ethics Subcommission of Universidad de La Sabana via Minute No. 011 of 2021; it was also approved by the institution where the sample was collected. All the participants agreed to be included in the study and signed the informed consent form. Environmental care measures were taken into account,
Results
The study population consisted of four groups, each one with 33 family members of patients hospitalized in an ICU from the city, therefore accounting for a total of 132 participants. The sociodemographic data can be consulted in Table 2
Table 2. Sociodemographic characterization by groups
X
Table 2. Sociodemographic characterization by groups
|
Experimental Group 1 |
Experimental Group 2 |
Control Group 1 |
Control Group 2 |
p-value |
| 33 | 33 | 33 | 33 |
| Age |
|
|
|
|
0.95 |
| 15-44 |
66.66 (22) |
60.60 (20) |
57.57 (19) |
63.63 (21) |
|
| 45-64 |
27.27 (9) |
30.30 (10) |
33.33 (11) |
30.30 (10) |
|
| ≥65 |
6.06 (2) |
9.09 (3) |
9.09 (3) |
6.06 (2) |
|
| Kinship with the patient |
|
|
|
|
0.13 |
| Father/Mother |
6.06% (2) |
9.09% (3) |
12.12% (4) |
12.12% (4) |
|
| Brother/Sister |
9.09% (3) |
9.09% (3) |
6.06% (2) |
18.18% (6) |
|
| Spouse |
66.66 (22) |
24.24% (8) |
24.24% (8) |
6.06% (2) |
|
| Son/Daughter |
60.61% (20) |
48.48% (16) |
39.39% (13) |
39.39% (13) |
|
| Other |
18.18% (6) |
9.09% (3) |
18.18% (6) |
24.24% (8) |
|
| Gender |
|
|
|
|
0.06 |
| Male |
9.09% (3) |
36.36% (12) |
30.30% (10) |
24.24% (8) |
|
| Female |
90.91% (30) |
63.63% (21) |
69.69% (23) |
75.75% (25) |
|
| Strata |
|
|
|
|
0.52 |
| Stratum 1 |
45.45% (15) |
42.42% (14) |
51.51% (17) |
63.63% (21) |
|
| Stratum 2 |
42.42% (14) |
48.48% (16) |
45.45% (15) |
27.27% (9) |
|
| Stratum 3 |
9.09% (3) |
9.09% (3) |
3.03% (1) |
9.09% (3) |
|
| Stratum 4 |
3.03% (1) |
0% (0) |
0% (0) |
0% (0) |
|
| Ocupation |
|
|
|
|
0.42 |
| Employee |
12.12% (4) |
18.18% (6) |
9.09% (3) |
6.06% (2) |
|
| Unemployed |
0% (0) |
3.03% (1) |
0% (0) |
3.03% (1) |
|
| Freelance worker |
15.15% (5) |
45.45% (15) |
36.36% (12) |
39.39% (13) |
|
| House chores |
63.63% (21) |
27.27% (9) |
51.51% (17) |
42.42% (14) |
|
| Retiree |
3.03% (1) |
3.03% (1) |
3.03% (1) |
3.03% (1) |
|
| Other |
6.06% (2) |
3.03% (1) |
0% (0) |
6.06% (2) |
|
| Schooling |
|
|
|
|
0.71 |
| Can read/write |
9.09% (3) |
3.03% (1) |
3.03% (1) |
9.09% (3) |
|
| Elementary School |
27.27% (9) |
27.27% (9) |
45.45% (15) |
36.36% (12) |
|
| High School |
42.42% (14) |
51.51% (17) |
39.39% (13) |
48.48% (16) |
|
| Technician/Technologist |
15.15% (5) |
12.12% (4) |
12.12% (4) |
6.06% (2) |
|
| Higher Education |
6.06% (2) |
6.06% (2) |
0% (0) |
0% (0) |
|
| Graduate Studies |
0% (0) |
0% (0) |
0% (0) |
0% (0) |
|
| Religión |
|
|
|
|
0.85 |
| Catholics |
93.93% (31) |
96.96% (32) |
93.93% (31) |
93.93% (31) |
|
| Protestants |
3.03% (1) |
3.03% (1) |
3.03% (1) |
6.06% (2) |
|
| Evangelical |
3.03% (1) |
0% (0) |
3.03% (1) |
0% (0) |
|
| Other |
0% (0) |
0% (0) |
0% (0) |
0% (0) |
|
| Marital Status |
|
|
|
|
0.74 |
| Single |
24.24% (8) |
18.18% (6) |
9.09% (3) |
24.24% (8) |
|
| Married |
21.21% (7) |
18.18% (6) |
36.36% (12) |
27.27% (9) |
|
| Consensual union |
42.42% (14) |
54.54% (18) |
51.51% (17) |
45.45% (15) |
|
| Separated/Divorced |
3.03% (1) |
3.03% (1) |
0% (0) |
0% (0) |
|
| Widowed |
9.09% (3) |
6.06% (2) |
3.03% (1) |
3.03% (1) |
|
| Baseline Uncertainty |
|
|
|
|
0.14** |
| Mean ± SD |
125 ±15 |
Not measured |
132 ±14 |
Not measured |
|
| Minimum - Maximum |
77 - 154 |
Not measured |
103 - 154 |
Not measured |
|
| Median |
125 |
Not measured |
128 |
Not measured |
|
| Final Uncertainty |
|
|
|
|
0.00** |
| Mean ± SD |
59 ±17 |
55 ±14 |
126 ±22 |
135 ±20 |
|
| Minimum - Maximum |
31 - 108 |
31 - 93 |
63 - 155 |
72 - 155 |
|
| Median |
62 |
59 |
121 |
143 |
|
*Fisher's Exact Test p<0.05: significant difference. **ANCOVA p<0.05: significant difference.
The participants' mean age was 41 years old, varying from 18 to 85; more than 63.62% in each group were women; 47% were the patients' children; and, regarding religion, Catholicism predominated with more than 93.92% in each group. More than 87.86% of the participant belonged to Stratus 2 or lower; with house chores ranking first in each group, followed by freelance workers, with the exception of the post-intervention Experimental group, where freelance workers prevailed, followed by house chores. In terms of schooling, more than 69.68% of the participants from each group have from Elementary to High School level. Regarding the participants' marital status, more than 42.41% in all groups are in consensual unions, followed by married individuals, as can be seen in Tabla 2. According to the aforementioned, no major difference between the groups is noticed.
The data obtained by the groups that were offered the Nursing intervention and conventional care are presented below (see Table 2).
Based on Table 2, it is noticed that the experimental groups presented high uncertainty with a mean Uncertainty Level (UL) = 125 points in the baseline assessments; in turn, they obtained low uncertainty with a mean UL <60 points. There is no larger difference in final uncertainty between the experimental groups, which might indicate that previous exposure (baseline assessment) to the form does not affect the result.
The following is observed in Table 2 regarding the control groups: they presented high uncertainty with a mean UL <125 points in the baseline and final assessments, respectively. In addition, they present very similar distributions, which might indicate that this does not affect the previous exposure result (baseline assessment) of the form.
The data obtained in the comparison between the effect of a Nursing intervention and conventional care on the uncertainty level in family members of people hospitalized in an ICU are presented below.
Uncertainty is classified according to its final score, as follows: low UL with <61 points, fair UL with 61-89 points; and high UL with >89 points14. The uncertainty classification across the experimental and control groups is presented below, according to the aforementioned categorization (see Table 3 ).
Table 3. Baseline and final uncertainty classification across the experimental and control groups
X
Table 3. Baseline and final uncertainty classification across the experimental and control groups
| Uncertainty Level |
Baseline uncertainty classification |
Final uncertainty classification |
| Experimental Group | Control Group | Experimental Group | Control Group |
| Low |
0% (0) |
0% (0) |
46.97% (31) |
0% (0) |
| Fair |
3,03% (1) |
0% (0) |
48.48% (32) |
4.55% (3) |
| High |
96,97% (32) |
100% (33) |
4.55% (3) |
95.45 (63) |
*Wilcoxon p: 0.001 Experimental Group. ** Wilcoxon p:0.100 Control Group.
Table 3; shows that baseline uncertainty is almost as high in the experimental group (96.97%) when compared to the control group. In turn, final uncertainty in the Experimental Group differs by 95.45% when compared to the Control Group; in this case, the Experimental Group reaches from fair to low uncertainty and the Control Group continues with uncertainty. Finally, it can be inferred that nearly 50% of the participants from the experimental group went from high to low uncertainty and that the rest dropped from high to fair uncertainty (see Figure 3).
Figure 3 shows that the Experimental Group presented a reduction of nearly 50% in final uncertainty when compared to the baseline value; in turn, final uncertainty slightly increased its mean value in the control groups, which allows inferring that the Nursing intervention reduces approximately 50% the uncertainty levels when compared to conventional care. In addition, receiving conventional care can generate an increase in the uncertainty level.
The central tendency measures observed for the experimental and control groups by each of the 4 subgroups are as follows: Experimental Group 1 starts with a mean uncertainty of 125 and ends with 59 (with a 66-point difference), whereas Control Group 1 has a baseline mean of 132 and ends with 126 (with a 6-point difference). There is a reduction in both groups; however, the one found in Experimental Group 1 exceeded 50%, whereas it was quite minimal in Control Group 1. In addition, it is noticed that Experimental Group 1 ends with a mean uncertainty of 59, whereas Experimental Group 2 ends with a mean of 55 and standard deviations of 17 and 14, respectively. It is also noticed that Control Group 1 ends with a mean uncertainty level of 126, whereas Control Group 2 ends with a mean of 136 and standard deviations of 22 and 20, respectively. This allows us to infer that the experimental and control groups present similar results; therefore, it would be necessary to resort to Solomon groups because there was no variation with prior knowledge about the uncertainty form.
The Shapiro-Wilk test indicates non-normal distributions; therefore, the hypothesis test is performed with Wilcoxon's, noticing that a statistically significant difference between baseline and final uncertainty is evidenced in Experimental Group 1 (p=0.001), which indicates that the intervention was effective; in turn, no significant differences are observed between baseline and final uncertainty in Control Group 1 (p=0.100).
Taking into account Mann-Whitney's U test, the distribution corresponding to final uncertainty is not statistically different either between the experimental groups (p=0.314) or in the control groups (p=0.078). Therefore, it is not necessary to resort to Solomon groups, and the results can only be differentiated with the final assessment.
Finally, the ANCOVA test was applied considering final uncertainty as dependent variable, Experimental Group 1 and Control Group 1 as independent variables and baseline uncertainty as their covariate; reasserting that there is a statistical difference (p=0.001) in the final uncertainty level among the experimental and control groups; in addition, it is evidenced that it is not necessary to consider any baseline assessment because there is no statistical difference: p=0.143.
Discussion
The study shows the effectiveness of the Nursing intervention for family members of patients hospitalized in an ICU on uncertainty, grounded on Merle Mishel's middle-range theory13. This research allows confirming the concepts of the theory and contributes more scientific knowledge about the phenomenon; in addition, the uncertainty level is significantly reduced in this study when compared to the family members that were offered conventional care.
Family members have their own care needs, which should be included in Nursing assistance as an integral care component4,14,15. The caregivers were mostly women, as can also be observed in different studies3,6,16-18. However, we also notice men emerging as caregivers, which slights reasserts the social change in terms of responsibility.
Given the above, it can be noticed that when their loved one is hospitalized, family members star to present different needs, especially regarding information, which is focused on their lack of knowledge about ICUs, their relative's health status, treatment and care they would be offered and whether they will survive, as is the case in the study by Taboada6. The aforementioned is worsened when family members lack any credible authority providing them proper education, taking into account how information is conveyed and the words used, among other details4.
By applying Merle Mishel's middle-range theory and its assessment scale for family members it was possible to easily evidence the phenomenon. The average-high baseline uncertainty levels are in line with other studies such as the one by Taboada and Inna6,7; in turn, they presented an average uncertainty level in the study by Massa3. However, this is attributed to the fact that it is a new event for the family members, reason why they lack proper tools to assign a clear meaning to the event6,13.
The results show that conventional care is not effective, reason why Nursing assistance should be started to be individualized according to each need6,9,19. This shows that a standardized intervention is more effective than conventional care.
The intervention was focused on the subconcepts of structure sources and on the concept of cognitive capabilities, in order to improve the family members' cognitive capacity with the aid of Nursing professionals as credible authorities and with continuing education. The aforementioned method was also used in part by Taboada and Zamora et al6,7, obtaining similarly favorable results.
The uncertainty level is always high when the first experiencing the event, as shown in this study6.
Taking into account the existence of the Hawthorne effect, the study was conducted following the Solomon group methodology, again asserting that the results obtained were not due to the agitation inherent in the family members for knowing what was being studied. This is because the results did not present any significant difference between the experimental groups, nor between the control groups.
Finally, it is important to note the major contribution offered by this study to the phenomenon of uncertainty in family members of patients hospitalized in Intensive Care Units for adults, so that standardized care continues to be replicated and acquires increasingly larger scales and duration in order to better enforce the fundamental right of families to be cared for as set forth in the Colombian political constitution20.
As a limitation, the participants present low schooling levels and belong to Stratus 2 or lower, reason why the instrument tended to be somewhat confusing for some people. In addition, the study was developed during the SARS-CoV-2 pandemic; therefore, it necessary to resort to technological aids not mastered by all people, besides having to comply with the mandatory social distancing.
Conclusions
It is concluded that the intervention is effective in reducing uncertainty among family members of patients hospitalized in an Intensive Care Unit from the city of Neiva, when compared to conventional care: p=0.001. In addition, as it was the first time that the family members had their loved one in an ICU, they presented very high uncertainty levels in all the groups subjected to the baseline assessment, which further reinforces the proposals set forth in Merle Mishel's middle-range theory. This is due to cognitive capacity and to the structure sources, where they initially lacked any credible authority and social support, in addition to their low knowledge about the ICU and their relative's health status.
It should also be considered that Solomon groups were used to avoid the Hawthorne effect, which indicated that the second assessment can be altered by the first one due to prior knowledge about the form. However, such effect was discarded, which indicates that the reduction in uncertainty is due to the intervention.
It is important to conclude that the family members presented higher uncertainty levels due to their limited knowledge about the event; therefore, their level will be high because it is their first time, reason why it would not be necessary to conduct baseline assessments or to use the Solomon group methodology in view of the results obtained.
New research studies in this area should continue to be carried out in the future, in order to keep strengthening the care provided to patients and family members in Intensive Care Units, hospitals and homes.
Limitations: This research was developed during the SARS-CoV-2 pandemic, reason why restrictions were faced for the entry of family members due to mandatory social distancing.
Conflict of interests: The authors declare having no conflict of interests.
Information related to funding: The project was funded by Universidad de La Sabana.
Acknowledgments: We would like to thank the health team, family members and patients from the institution where the study was conducted.
References
X
Referencias
Koulouras V, Konstanti Z, Lepida D, Papathanakos G, Gouva M. Shame feeling in the Intensive Care Unit patient’s family members. Intensive Crit Care Nurs. 2017;41:84-9 https://doi.org/10.1016/j.iccn.2017.03.011
X
Referencias
Massa ER, Torres IEF, Prieto AMPM. Incertidumbre en cuidadores familiares de pacientes hospitalizados en unidades de cuidado intensivo. Investig En Enferm Imagen Desarro. 2018;20(1). https://doi.org/10.11144/Javeriana.ie20-1.icfp
X
Referencias
Cabete D dos SG, da Fonte CS, de Matos MMS, Patrica HM, Silva ARR, de Abranches Silva VFV. Emotional support to the family of the critically ill patient: nursing interventions. Rev Enferm Referência. 2019;4(20):129-37. https://doi.org/10.12707/RIV18062
X
Referencias
Mishel MH, Epstein D. Uncertainty in illness scales manual. Chapel Hill NC Univ N C. 1997;4-9.
X
Referencias
Taboada Suarez JE. Intervención de enfermería fundamentada en la comunicación sobre la incertidumbre de familiares de pacientes hospitalizados en la UCI adultos [Tesis maestría en Enfermería] Bogotá. Universidad de La Sabana; 2019.http://hdl.handle.net/10818/35589
X
Referencias
Zamora-Córdova M, Meza-Curo O, Juárez-Ramos E, Salazar-Cárdenas M. Efecto de un programa educativo en el conocimiento y la incertidumbre de los familiares de pacientes en unidad de cuidados intensivos materna. Rev Peru Investig Materno Perinat. 2019;8(3):21-6. https://doi.org/10.33421/inmp.2019161
X
Referencias
Smith MJ, Liehr PR. Middle range theory for nursing. Nueva York Springer Publishing Company; 2018.
X
Referencias
Padilla Fortunatti CF. Most important needs of family members of critical patients in light of the critical care family needs inventory. Investig Educ En Enfermeria. 2014;32(2):306-16. https://doi.org/10.17533/udea.iee.v32n2a13
X
Referencias
Desu M. Sample size methodology. Nueva York Elsevier; 2012.
X
Referencias
Perez Campos, Diego Omar. (2023). “Base de datos. Efecto de una intervención enfermera sobre: incertidumbre de familiares en Cuidado Intensivo”, Mendeley Data, V1. https://doi.org/10.17632/txdkt9gdr7.1
X
Referencias
Castillo Culquerricra M. Necesidades de los familiares de pacientes internados en unidad de cuidado intensivo del Hospital Regional Virgen de Fátima Chachapoyas, 2017. [Tesis licenciatura en enfermería] Perú. Universidad Nacional Toribio Rodríguez de Mendoza de Amazonas; 2017. https://hdl.handle.net/20.500.14077/1156
X
Referencias
Kang J, Cho YJ, Choi S. State anxiety, uncertainty in illness, and needs of family members of critically ill patients and their experiences with family-centered multidisciplinary rounds: A mixed model study. Plos One. 2020;15(6):e0234296.
X
Referencias
Bautista Rodríguez LM, Arias Velandia MF, Carreño Leiva ZO. Percepción de los familiares de pacientes críticos hospitalizados respecto a la comunicación y apoyo emocional. Rev Cuid. 2016;7(2):1297-1309.https://doi.org/10.15649/cuidarte.v7i2.330
-
Diez VBH, Gorris M del PS, Romano EB, Gracia CM, Elía LT, Sancho CP. Necesidades de la familia del paciente crítico en la unidad de cuidados intensivos. Rev Sanit Investig. 2022;3(2):27 https://revistasanitariadeinvestigacion.com/necesidades-de-la-familia-del-paciente-critico-en-la-unidad-de-cuidados-intensivos/
-
Koulouras V, Konstanti Z, Lepida D, Papathanakos G, Gouva M. Shame feeling in the Intensive Care Unit patient’s family members. Intensive Crit Care Nurs. 2017;41:84-9 https://doi.org/10.1016/j.iccn.2017.03.011
-
Massa ER, Torres IEF, Prieto AMPM. Incertidumbre en cuidadores familiares de pacientes hospitalizados en unidades de cuidado intensivo. Investig En Enferm Imagen Desarro. 2018;20(1). https://doi.org/10.11144/Javeriana.ie20-1.icfp
-
Cabete D dos SG, da Fonte CS, de Matos MMS, Patrica HM, Silva ARR, de Abranches Silva VFV. Emotional support to the family of the critically ill patient: nursing interventions. Rev Enferm Referência. 2019;4(20):129-37. https://doi.org/10.12707/RIV18062
-
Mishel MH, Epstein D. Uncertainty in illness scales manual. Chapel Hill NC Univ N C. 1997;4-9.
-
Taboada Suarez JE. Intervención de enfermería fundamentada en la comunicación sobre la incertidumbre de familiares de pacientes hospitalizados en la UCI adultos [Tesis maestría en Enfermería] Bogotá. Universidad de La Sabana; 2019.http://hdl.handle.net/10818/35589
-
Zamora-Córdova M, Meza-Curo O, Juárez-Ramos E, Salazar-Cárdenas M. Efecto de un programa educativo en el conocimiento y la incertidumbre de los familiares de pacientes en unidad de cuidados intensivos materna. Rev Peru Investig Materno Perinat. 2019;8(3):21-6. https://doi.org/10.33421/inmp.2019161
-
Smith MJ, Liehr PR. Middle range theory for nursing. Nueva York Springer Publishing Company; 2018.
-
Raurell AA, Aymar IM. Necesidad de rol en los familiares del paciente en la unidad de cuidados intensivos. Enferm Intensiva. 2015;26(3):101-11. https://doi.org/10.1016/j.enfi.2015.02.001
-
Padilla Fortunatti CF. Most important needs of family members of critical patients in light of the critical care family needs inventory. Investig Educ En Enfermeria. 2014;32(2):306-16. https://doi.org/10.17533/udea.iee.v32n2a13
-
Desu M. Sample size methodology. Nueva York Elsevier; 2012.
-
Whittemore R, Grey M. The systematic development of nursing interventions. J Nurs Scholarsh. 2002;34(2):115-20.https://doi.org/10.1111/j.1547-5069.2002.00115.x
-
Perez Campos, Diego Omar. (2023). “Base de datos. Efecto de una intervención enfermera sobre: incertidumbre de familiares en Cuidado Intensivo”, Mendeley Data, V1. https://doi.org/10.17632/txdkt9gdr7.1
-
Ministerio de Salud, República de Colombia. Resolución No. 8430, octubre 4, por la cual se establecen las normas científicas, técnicas y administrativas para la investigación en salud. 1993 [Internet]. Bogotá D.C. Consulta: diciembre 12, 2023. Disponible en: https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/DE/DIJ/RESOLUCION-8430-DE-1993.PDF
-
Castillo Culquerricra M. Necesidades de los familiares de pacientes internados en unidad de cuidado intensivo del Hospital Regional Virgen de Fátima Chachapoyas, 2017. [Tesis licenciatura en enfermería] Perú. Universidad Nacional Toribio Rodríguez de Mendoza de Amazonas; 2017. https://hdl.handle.net/20.500.14077/1156
-
Kang J, Cho YJ, Choi S. State anxiety, uncertainty in illness, and needs of family members of critically ill patients and their experiences with family-centered multidisciplinary rounds: A mixed model study. Plos One. 2020;15(6):e0234296.
-
Mishel MH. Uncertainty in illness. Image J Nurs Sch. 1988;20(4):225-32. https://doi.org/10.1111/j.1547-5069.1988.tb00082.x
-
Bernal-Ruiz D, Horta-Buitrago S. Cuidado de enfermería para la familia del paciente crítico desde la teoría de la comprensión facilitada. Enferm Univ. 2014;11(4):154-63. https://doi.org/10.1016/S1665-7063(14)70928-5
-
Bautista Rodríguez LM, Arias Velandia MF, Carreño Leiva ZO. Percepción de los familiares de pacientes críticos hospitalizados respecto a la comunicación y apoyo emocional. Rev Cuid. 2016;7(2):1297-1309.https://doi.org/10.15649/cuidarte.v7i2.330
-
Republica de Colombia. Constitución política de Colombia. 1991 [Internet] Bogotá. Consulta: diciembre 12, 2023. Disponible en: https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/INEC/IGUB/constitucion-1991.pdf