Rev Cuid. 2025; 16(3): e4510
Abstract
Introduction: Work overload is associated with missed care and a higher prevalence of adverse events.
The study aims to generate empirical evidence on nursing workload in intensive care units in Colombia,
considering differences in team composition based on qualifications, skills, and competencies (Skill Mix).
Objective: To compare the workload and distribution of nursing activities in two intensive care units
with different Nursing Care Models based on the application of the TISS-28.
Materials and Methods: Quantitative and retrospective study with data from medical records of patients
treated between 2018 and 2020 in Medellín. The TISS-28 was calculated upon admission and SAPS-3 was used
to control for confounding variables. Mean and proportion comparison tests were used according to the type
of variable and data distribution pattern.
Results: The nurses in both ICUs had a patient assignment higher than indicated by the TISS-28.
Surgical patients, those with vasoactive drugs, transfusions, adverse events, or those who died,
had longer care times. The adverse events increased proportionally with the TISS-28 level.
Discussion: Key elements include the relationship between care safety and staff qualification,
experience and workload; the missed nursing care; and the undervaluation of care as a public good.
Conclusions: It was identified that in both ICUs there is a higher workload for nurses regarding
the time available for activities and patients. The majority of care provided by the nursing assistants
in the ICU2-Assistants do not correspond with their level of training and legal responsibility.
Keywords:
Critical Care Nursing; Hospital Nursing Staff; Nurses; Nursing Assistants; Workload.
Resumen
Introducción: La sobrecarga de trabajo se asocia con la omisión del cuidado y mayor prevalencia de Eventos Adversos.
El estudio pretende generar evidencia empírica sobre la carga de enfermería en unidades de cuidado intensivo en Colombia
con diferencias en la composición del equipo por cualificaciones, habilidades y competencias (Skill Mix).
Objetivo: Comparar la carga de trabajo y la distribución de actividades de enfermería en dos UCI con diferentes
Modelos de Atención de Enfermería basados en la aplicación del TISS-28.
Materiales y Métodos: Estudio cuantitativo y retrospectivo con datos de atenciones clínicas entre 2018 y 2020 en Medellín.
Se calculó el TISS-28 al ingreso y se usó Simplified Acute Physiology Score 3 (SAPS-3) para controlar variables confusoras.
Se utilizaron pruebas de comparación de medias y proporciones según el tipo de variable y patrón de distribución de los datos.
Resultados: La asignación de pacientes en ambas UCI fue superior a la recomendada indicada por el TISS-28.
Los pacientes quirúrgicos, con vasoactivos, transfusiones, eventos adversos (EA) o que murieron requirieron mayores tiempos de cuidado.
Los EA aumentaron de forma proporcional con el nivel del TISS-28.
Discusión: Destacan elementos como la relación entre la seguridad del cuidado y el nivel de formación, experiencia del personal
y carga de trabajo; la omisión de cuidados y la subvaloración del cuidado como bien público.
Conclusiones: Se identificó que en ambas UCI hay más carga de trabajo para las enfermeras respecto al tiempo disponible
por actividades y pacientes. La mayor parte de cuidados brindados por las auxiliares de enfermería de la UCI2-Auxiliares
no corresponden con su nivel de formación y de responsabilidad legal.
Palabras Clave:
Enfermería de Cuidados Críticos; Personal de Enfermería en Hospital; Enfermeras; Asistentes de Enfermería; Carga de Trabajo.
Resumo
Introdução: A sobrecarga de trabalho está associada à negligência dos cuidados e à maior prevalência
de eventos adversos. Este estudo tem como objetivo gerar evidências empíricas sobre a carga de trabalho
de enfermagem em unidades de terapia intensiva na Colômbia, com diferenças na composição da equipe por
qualificações, habilidades e competências (Skill Mix).
Objetivo: Comparar a carga de trabalho e a distribuição das atividades de enfermagem em duas UTIs
com diferentes Modelos de Assistência de Enfermagem, a partir da aplicação do TISS-28.
Materiais e Métodos: Estudo quantitativo e retrospectivo com dados de atendimentos clínicos entre
2018 e 2020 em Medellín. O TISS-28 foi calculado na admissão, e o Simplified Acute Physiology Score 3 (SAPS-3)
foi utilizado para controlar variáveis de confusão. Testes de comparação de médias e proporções foram utilizados
de acordo com o tipo de variável e o padrão de distribuição dos dados.
Resultados: A alocação de pacientes em ambas as UTIs foram maiores do que a indicada pelo TISS-28.
Pacientes submetidos a cirurgias, agentes vasoativos, transfusões, eventos adversos (EA) ou óbitos necessitaram
de maior tempo de cuidado. Os EA aumentaram proporcionalmente com a pontuação do TISS-28.
Discussão: Os elementos destacados incluem a relação entre a segurança do cuidado e o nível de
treinamento, experiência da equipe e carga de trabalho; a omissão de cuidado; e a subvalorização do cuidado
como um bem público.
Conclusões: Foi identificado que, em ambas as UTIs, os enfermeiros têm maior carga de trabalho
em comparação ao tempo disponível para atividades e pacientes. A maioria dos cuidados prestados pelos
auxiliares de enfermagem na UTI2-Auxiliares não corresponde ao seu nível de treinamento e responsabilidade legal.
Palavras-Chave:
Enfermagem de Cuidados Críticos; Pessoal de Enfermagem em Hospital; Enfermeiras; Assistentes de Enfermagem; Carga de Trabalho.
Introduction
The quality of care and the clinical outcomes of patients are related to the ways in which nursing staff
organize their work – represented in Nursing Care Models (NCMs) – however, there is little clarity on
the ideal allocation of workload for such staff, especially because it is affected by different attributes
such as the amount of nursing time and functions assigned, the level of knowledge and skills, the
complexity of care, the weight of the intensity of care and the physical, mental and emotional effort
1-3.
Workload analysis allows nursing managers to calculate staffing and patient allocation in the Intensive
Care Unit (ICU) considering the needs of each patient and the severity of their health condition
4-5.
Scientific literature shows that assigning nursing teams to patient care without determining the
workload with validated instruments is correlated with decreased quality of care and patient safety,
expressed in indicators such as adverse events (AEs) in the ICU, and omission of care
6-7.
Research conducted in Egypt, Western Australia, South Korea, and Brazil showed a positive
correlation between workload and neglect of care, due to the high number of patients per nurse,
poor infrastructure, and staff with multiple employment contracts
6-9.
In contrast, research focused on identifying the association between the use of nursing aids and
nurse-patient outcomes showed that implementing a mandatory minimum nurse-to-patient ratio
8
was associated with or correlated with improvements in indicators such as job satisfaction and a
reduction in adverse events such as healthcare-associated infections, pressure ulcers, and patient
falls
10.
In Colombia, the study by Arango was found
11,
whose correlation analyses were inconclusive in establishing a correlation between patient allocation
and some indicators of quality of healthcare. A group of studies with design limitations was also
identified, such as setting comparative objectives but presenting unified results without
disaggregating any group
12,
proposing descriptive approaches without establishing relationships between variables
13,
applying statistical tests that do not correspond to the data distribution pattern, the
quantitative-qualitative nature of the information, or the data tabulation method (e.g., applying
Student’s t-tests to compare three data groups)
5.
Regarding the nurse-patient ratio, territories such as the United States, the United Kingdom, and
Australia have established 1:1 standards for ICUs
14;
however, the regulations of the Colombian health system have not established a nurse-patient
ratio, and therefore, hospitals consider hiring nursing technicians for the direct care of patients
under the supervision of a nurse per ward, who has legal responsibility for patient care and also
performs administrative functions
1,15.
Adding to this situation is the limited availability of nurses and inequities in their geographical
distribution, as they are mostly concentrated in large urban centers
16.
In Colombian ICUs, there is a greater availability of nurses for direct care compared to inpatient
services due to technological complexity and patient care requirements. However, workload overload
has been observed related to the limited availability of nurses, the number of duties, and the
severity of the patients assigned
17.
A heterogeneous range of nurse-patient assignments has been found, ranging from 1-3, allowing
nurses to participate in direct patient care, to 1-12, where the nurse is limited to ward management
and loses the central role in patient care, delegating all care to the nursing assistants under their
supervision
18.
Regarding the distribution of tasks, Arango
11
describes that nurses perform few direct care activities, mainly medication administration and
transfusion supervision. The rest of their time is spent on administrative tasks, and most of the care
is provided by nursing assistants without the technical and legal competence for the functions they
perform.
Given the lack of regulations on the nurse-to-patient ratio, the use of validated instruments such as
the Therapeutic Intervention Scoring System (TISS-28) allows nursing managers to calculate workloads
and assign nursing teams according to the severity level and care requirements of patients
13,19.
One aspect to highlight is that the different studies reviewed in Colombia agree in showing the work
overload on nursing staff, although none of them provides a description of the workload in relation to
the composition of the work teams by levels of qualifications, skills and competencies (Skill Mix) and
the distribution of activities of the TISS-28
5,11,12,20.
Considering the methodological limitations of some of the studies carried out in the Colombian
context, the heterogeneity in the nurse-patient ratio and the diffuse and unregulated boundaries on
the functions of nurses and nursing assistants in hospital care, the development of local knowledge
is required that integrates these factors in a relational way and generates knowledge for action, that
is, studies with epistemic vigilance on the methodological rigor itself and that study the workload in
ideal scenarios regarding the allocation of patients and functions between nurses and nursing
assistants.
Given the need to establish nurse-patient assignments that align with care needs, some Colombian
hospitals have made progress in implementing Nursing Care Models (NCMs) with a higher proportion
of registered nurses, fewer assigned patients, and a distinction in the roles of nurses and nursing
assistants based on their qualifications and legal responsibilities: nurses for direct care and auxiliary
staff for comfort support activities. Analyses of workloads in these new NCMs are limited, making
them an emerging field for research on the relationship between workload, roles, and quality of
nursing care
19.
This led to an interest in conducting a comparative study in two Intensive Care Units (ICUs) of a high-
complexity hospital in Medellín, Colombia, with different organizational structures for their nursing
teams. In one ICU, nurses provide direct care with support from nursing technicians for comfort care
activities, while in the second ICU, a nurse is responsible for the ward and supervises the nursing
technicians, who provide most of the patient care, including tasks for which they lack the necessary
skills, such as medication administration, infusion preparation, and some invasive procedures. The
units differ in the proportion of nurses and nursing assistants per team, the number of patients, and
their assigned roles. To identify similarities or differences in workload under these organizational
structures of nursing care, the following study objective was established: to compare the workload
and distribution of nursing activities in two ICUs with different Nursing Care Models based on the
application of the TISS-28.
Materials and Methods
The design and location of the study
This quantitative, descriptive, and retrospective study used data from the medical records of patients
in two ICUs at a hospital in Medellín between December 2018 and March 2020, a period corresponding
to the institutional piloting of two nursing care models for adult ICUs. The ICUs differed in the
composition, skills, and functions within their nursing teams and were designated ICU1-Nurses and
ICU2-Nursing Assistants, based on the profile that was more numerous and performed the greatest
proportion of direct patient care in each ICU.
Population
One thousand Electronic Health Records (EHRs) of patients over 18 years of age, with a hospital stay
longer than 48 hours and with a single admission to the ICU during their hospital stay, were included.
For the sample size calculation, the average number of adverse events (AEs) in each ICU between
January 2018 and August 2019 was used, with a standard deviation (SD), a power of 90%, a type of
alpha error of 5%, and an adjustment for losses of 20%, determining a minimum of 348 admissions in
each group.
Variables, instruments, and data collection procedures
A data collection protocol was in place for reviewing medical records, applying instruments, and
training the data collection personnel. Data collection took place between July 2021 and June
2023. Sociodemographic variables of the patients were collected, as well as adverse events (AEs)
experienced during their ICU stay. The probability of death, and the duration and care requirements
based on the severity of the patient's condition during the first day of ICU stay, were calculated using
the Simplified Acute Physiology Score (SAPS-3). Therapeutic Intervention Score System TISS-28, both
validated for the Colombian and South American context
20.
The TISS-28 has six domains: basic activities, ventilatory support, cardiovascular support, renal support,
neurological and metabolic support, and specific interventions
21,22.
The total score can range from 0 to 76 points and classifies patients into four severity levels, each with a
specific nurse-to-patient ratio: Class I with a 1:4 ratio; Class II 1:4; Class III 1:2; and Class IV with a 1:1
or 2:1 nurse-to-patient ratio. Classes I and II require observation or active monitoring, while Classes III
and IV require intensive care and therapy
21.
Data analysis
For qualitative variables, absolute and relative frequencies were calculated, and for quantitative
variables, measures of central tendency and dispersion were calculated. Once normality in the
distribution of the variables was determined, chi-square tests and corresponding mean comparison
tests were performed. The data included both within-group and between-group comparisons. All
collected data are freely available for access and consultation on Mendeley Data
23.
Validity criteria
To ensure internal validity, a protocol was developed using validated instruments, and the data
collection staff was trained and supervised. Weekly audits were conducted, and the quality of 20%
of the medical records collected was analyzed. The SAPS-3 was used to ensure patient comparability
and control for confounding biases related to demographic and clinical characteristics.
Ethical considerations
This research was deemed safe according to Colombian Resolution 8430/1993. Approval was obtained
from an Ethics Committee (CEI-FE 2019 minutes), adhering to the legal confidentiality criteria of the
HCL. The confidentiality of the hospital's name was guaranteed, as well as the anonymized use of
sensitive patient information using alphanumeric identification codes and the removal of variables
such as name and identification number.
Results
Characteristics of the nursing staff participating in ICUs
The main differentiating characteristic of the working methods in the ICUs compared is skill staffing
mix (proportion of professional staff on teams and assignment of roles). The proportion of nurses
in ICU 1-Nurses is three times greater than in ICU 2-Nursing Assistants. In ICU 1-Nurses, one nurse
is responsible for three patients and one nursing assistant for four patients. There are four nurses
and three nursing assistants per shift to cover the unit's 12 beds, in addition to an administrative
coordinator on day shifts and weekdays, who oversees the service's administrative management
(Table 1). In ICU 2-Nursing Assistants, there is one nurse per shift, responsible for the care of 13
patients, with six nursing assistants, most of whom care for two patients (Table 1).
The distribution described places the nurses in ICU1-Nurses in a direct care role with support from
nursing assistants for comfort activities, while in ICU2-Auxiliaries the nurse has a management-
administration profile of the ward and delegates most of the care to the nursing assistants, except for
taking blood cultures and assisting in invasive procedures.
Table 1. Characterization of nursing staff and ICUs compared
X
Table 1. Characterization of nursing staff and ICUs compared
| ICU variables |
ICU 1 Nurses |
ICU 2 Assistants |
| Nursing staff allocation per patient |
|
|
| Nurses |
1:3 |
1:13 |
| Assistants |
1:4 |
1:2 |
| Available beds |
12 |
13 |
| Number of staff per shift |
|
|
| Nurses |
4 |
1 |
| Assistants |
3 |
6 |
| Coordinator |
1 |
0 |
| Rotating bed |
7.44 days / patient |
9.24 days / patient |
|
|
|
| Nursing variables |
ICU 1 Nurses |
ICU 2 Assistants |
|
n Median (IQR) |
n Median (IQR) p-value |
| Age (years) |
|
|
| Assistants |
7 23 (4) |
17 33 (7) <0.001* |
| Nurses |
17 34 (13) |
5 30 (8) 0.249* |
| Years of experience |
|
|
| Assistants |
7 3 (0.0) |
17 5 (7.5) 0.494* |
| Nurses |
17 3 (10.5) |
5 1 (1.5) 0.002* |
| Skill Mix n [%] |
|
0.005~ |
| Assistant |
7 [29.20] |
17 [77.30] |
| Nurse |
9 [37.50] |
3 [13.60] |
| Specialist |
8 [33.30] |
2 [9.10] |
ICU – Intensive Care Unit, IQR – Interquartile range,
~ p value for chi square, * p value for Mann's U Whitney.
The sociodemographic characteristics of the work teams show that in ICU 1-Nurses, the nurses are
older and have similar professional experience compared to the nursing assistants (Table 1), while
in ICU 2-Assistants, the auxiliary staff are older and have more experience. The dispersion measures
for years of experience suggest that within the teams, there is a coexistence of highly experienced
individuals and a constant turnover of new staff with little work experience. The bed turnover rate
indicates longer hospital stays in ICU 2-Assistants.
Patient characteristics and workload according to TISS-28
In the two ICUs compared, a similar mean age was found, along with a higher proportion of men
and discharges. Patients did not show significant differences in their demographic and clinical
characteristics, except for the proportion of scheduled admissions, surgical and cardiovascular
patients, and the time spent on the TISS-28, suggesting that patients in ICU 1-Nurses had greater
care requirements. A direct proportional increase was also found between the TISS-28 level and the
percentage of adverse events, which were significantly higher for ICU 2-Auxiliaries (Table 2).
Table 2. Characteristics of patients treated during the study period. n=1000
X
Table 2. Characteristics of patients treated during the study period. n=1000
| Variable |
ICU 1 Nurses
% (n)
541 |
ICU 2 Assistants
% (n)
459 |
p-value |
| Sex |
|
|
0.689* |
| Male |
55.82 (302) |
57.08 (262) |
|
| Female |
44.18 (239) |
42.92 (197) |
|
| Age (years) - Mean ± SD |
52 ± 19.70 |
52.4 ± 19.10 |
0.856~ |
| Type of income |
|
|
<0.001* |
| Programmed |
22.92 (124) |
13.73 (63) |
|
| Urgent |
77.08 (417) |
86.27 (396) |
|
| Type of discharge |
|
|
0.255* |
| High |
85.95 (465) |
82.14 (377) |
|
| Death |
14.05 (76) |
17.86 (82) |
|
| Probability of death |
|
|
0.854~ |
| SAPS 3 (%) |
47.80 (NA) |
48.10 (NA) |
|
| Health regimen |
|
|
0.44 |
| Contributory |
41.04 (222) |
37.47 (172) |
|
| Subsidized |
53.60 (290) |
55.99 (257) |
|
| Not affiliated |
5.36 (29) |
6.54 (30) |
|
| Place of origin |
|
|
0.03 |
| Emergency room, another hospital |
59.10 (320) |
65.80 (302) |
|
| Another place in the hospital |
40.85 (221) |
34.20 (157) |
|
| Days of hospitalization prior to admission to the ICU |
|
|
0.18 |
| 0 to 13 days |
93.16 (504) |
95.86 (440) |
|
| 14 to 27 days |
5.36 (29) |
3.27 (15) |
|
| Greater than or equal to 28 days |
1.48 (8) |
0.87 (4) |
|
| Admitted for digestive pathology |
|
|
0.86 |
| No |
89.54 (479) |
88.89 (408) |
|
| Yes |
11.46 (62) |
11.11 (51) |
|
| Admitted for a liver condition. |
|
|
0.94 |
| No |
97.97 (530) |
98.04 (450) |
|
| Yes |
2.03 (11) |
1.96 (9.00) |
|
| Admitted for a neurological condition. |
|
|
0.14 |
| No |
60.63 (328) |
65.14 (299) |
|
| Yes |
39.37 (213) |
34.86 (160) |
|
| Admitted for surgery |
|
|
<0.001 |
| Programmed |
22.92 (124) |
15.47 (71) |
|
| Urgent |
29.57 (160) |
21.35 (98) |
|
| Non-surgical |
47.50 (257) |
63.18 (290) |
|
| Admitted for cardiovascular pathology |
|
|
0.01 |
| No |
78.19 (423) |
70.37 (323) |
|
| Yes |
21.81 (118) |
29.63 (136) |
|
| TISS Average 28 |
|
|
0.003~ |
| Mean Score ± SD |
32 ± 9.10 |
30.2 ± 9.10 |
|
| TISS Category 28 |
|
|
0.011* |
| II = 10-19 points |
9.43 (51) |
13.51 (62) |
|
| III = 20-39 points |
67.28 (364) |
69.72 (320) |
|
| IV => 40 points |
23.29 (126) |
16.78 (77) |
|
| Minutes of care required Mean ± SD |
330 ± 94.30 |
309.00 ± 93.70 |
<0.001~ |
| Adverse events by TISS-28 category |
|
|
<0.001* |
| II |
25.50 (13) |
38.70 (24) |
|
| III |
56.90 (207) |
66.90 (214) |
|
| IV |
85.70 (108) |
92.20 (71) |
|
ICU-Intensive Care Unit, SD-Standard Deviation, SAPS 3-Simplified Acute Physiology Score,
TISS 28-Simplified Therapeutic Intervention Score System,
* p-value for chi square ~ p-value for Mann Whitney U.
Applying the TISS-28 to patient medical records resulted in a slightly higher overall average and care
time in the ICU1-Nurses unit. Regarding severity level, approximately 70% of patients were classified
as TISS-28 category 3. Patient assignments to nursing assistants in both ICUs corresponded to the ideal
assignment calculated using the TISS-28, while for nurses, it revealed work overload; consequently,
the number of patients assigned exceeded the ideal value based on the TISS-28 (Table 3).
Table 3: Care times, nursing staff-patient ratio and proportion of patients by TISS-28 categories
X
Table 3: Care times, nursing staff-patient ratio and proportion of patients by TISS-28 categories
TISS-28
Category |
Job profile |
Median [IQR]
minutes of care required |
Staff-to-patient ratio |
Patients treated
% (n) |
Median [IQR]
minutes of care required |
Staff-to-patient ratio |
Patients treated
% (n) |
| Ideal TISS-28 |
Real |
Ideal TISS-28 |
Real |
|
|
|
ICU 1 Nurses |
ICU 2 Assistants |
|
| 2 |
Nurse |
101 [60-145] |
1:5 |
1:3 |
9.40 (51) |
42 [32-99] |
1:11 |
1:13 |
13.50 (62) |
| AN |
54 [53-80] |
1:9 |
1:4 |
108 [81-152] |
1:4 |
1:2 |
| 3 |
Nurse |
222 [116-318] |
1:2 |
1:3 |
67.30 (364) |
112 [47-190] |
1:4 |
1:13 |
69.70 (320) |
| AN |
96 [53-113] |
1:5 |
1:4 |
192 [112-281] |
1:2 |
1:2 |
| 4 |
Nurse |
337 [294-447] |
1:1 |
1:3 |
23.30 (126) |
184 [150-219] |
1:3 |
1:13 |
16.80 (77) |
| AN |
108 [92-125] |
1:4 |
1:4 |
258 [212-312] |
1:2 |
1:2 |
ICU-Intensive Care Unit, IQR-interquartile range,
TISS 28-Simplified Therapeutic Intervention Score System,
AN-Auxiliary nurse.
Distribution of functions and care times according to TISS-28 activities
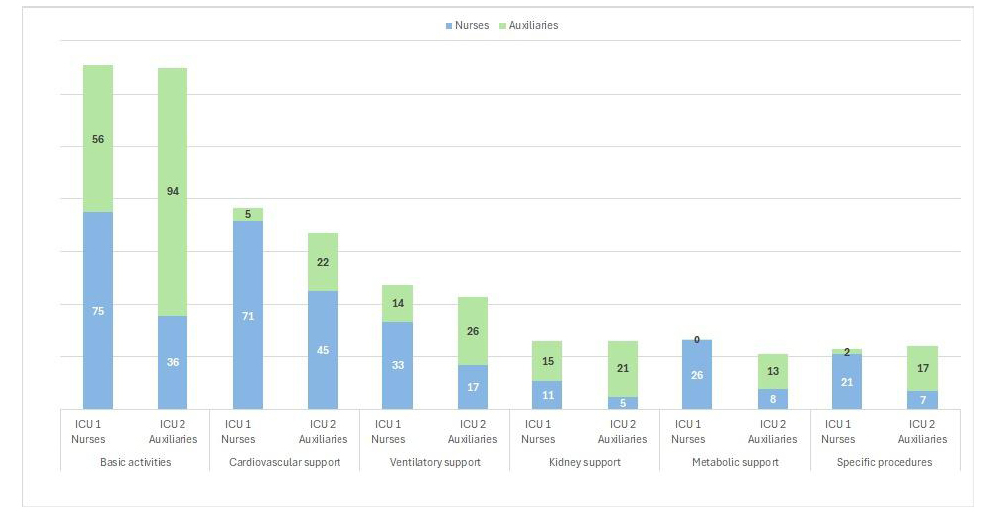
When analyzing care time across the six activity groups distributed between nurses and nursing
assistants, it was observed that basic care consumed the most time, followed by cardiovascular and
ventilatory support in both units. In ICU 1-Nurses, the nurse had the greatest involvement in all care
activities, while in ICU 2-Assistants, it was the nursing assistants, except for cardiovascular support
activities, where the nurse was more involved (Figure 1).
The analysis of specific activities of the TISS-28 shows that in the ICU1-Nurses, nurses perform
activities such as the administration of medications and vasoactive drugs, ventilatory support,
invasive procedures such as taking laboratory samples, nutritional support, the management of
wound care, drains and catheters, CPR and assistance to intra-ICU procedures, while the nursing
assistant has greater participation in activities such as patient monitoring, fluid balance and actions
not contemplated in the TISS-28 such as assistance in basic activities of daily living.
In the case of the ICU2-Auxiliary Unit, the nurse performs invasive procedures such as the management
of catheters, complex wound care, sample collection, and assistance with intra-ICU medical
procedures, while nursing assistants provide assistance with activities of daily living and additionally
offer care such as medication administration, management of metabolic complications, nutritional
support, ventilatory support, and artificial airway management (Figure 1).
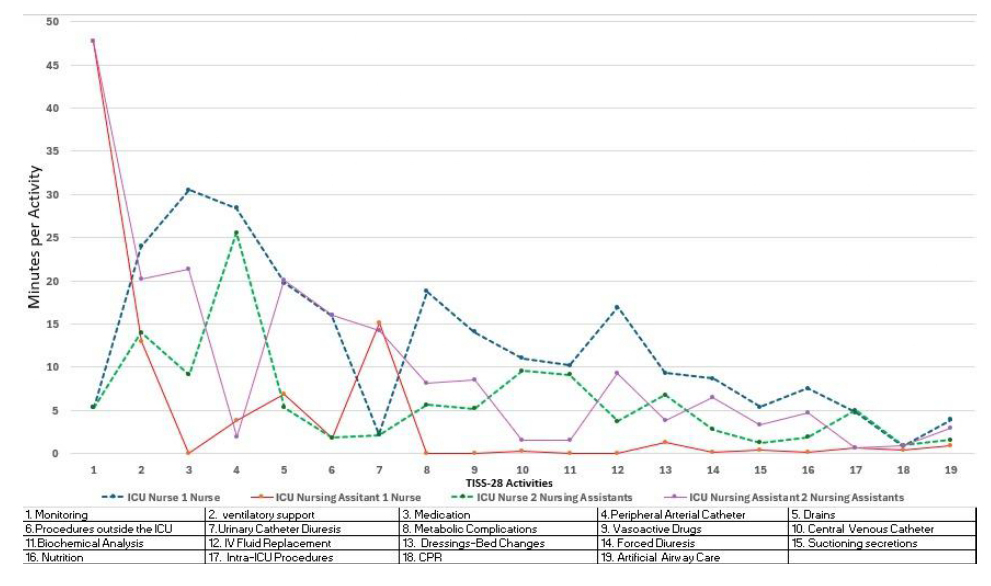
Figure 2 shows three trends regarding the care provided by nurses and nursing assistants in the two
ICUs. The first trend reveals a similarity in the functions and roles of both nursing assistants and nurses
in both ICUs, in activities such as bladder catheterization, management of peripheral and central
arterial catheters, wound care and bed changes, biochemical analysis, and intra-ICU procedures
(activities 4,7,10,11,13,17). This suggests an equivalence in the responsibilities and tasks between the
staff of the ICUs compared.
The second trend highlights that nursing assistants in ICU2 (Auxiliaries) perform the same functions
as nurses in ICU1 (Nurses), namely, ventilatory support, medication administration, drainage
management, secretion suctioning, artificial airway management, nutrition, and procedures outside
the ICU (activities 2,3,5,6,15,16,19). This finding indicates a redistribution of roles where nursing
assistants in ICU2 (Auxiliaries) assume responsibilities that would normally be reserved for nurses in
ICU1 (Nurses).
In the third trend, the functions of biochemical analysis, nutrition, medication administration,
management of metabolic complications and central venous catheters, fluid balance, vasoactive
agents, and forced diuresis are restricted for nursing assistants in the ICU-Nurses unit and are performed
by registered nurses (activities 3,8,10,11,16). This restriction is in place to ensure that nursing assistants
do not perform functions outside their technical competence and legal responsibility.
Regarding the average length of care required according to the patients' sociodemographic and clinical
characteristics (Table 4), significant differences were found indicating that patients who underwent
surgery, used vasoactive drugs prior to ICU admission, received intra-ICU blood transfusions,
experienced adverse events, or died, required longer care times in both ICUs. Differences in care times
by TISS-28 severity level were also significant in both ICUs (p < 0.001).
Table 4: TISS-28 care time required according to patient characteristics
X
Table 4: TISS-28 care time required according to patient characteristics
| Variables |
ICU 1 Nurses
Average ± SD |
p-value |
ICU 2 Assistants
Average ± SD |
p-value |
| Sex |
| 0.877 | | 0.919 |
| Women |
330.5 ± 101.63 |
|
309.53 ± 97.93 |
|
| Man |
330.15 ± 88.41 |
|
309.96 ± 90.65 |
|
| Age range in years* |
| 0.294 | | 0.056 |
| <40 |
323.03 ± 85.73 |
|
308.82 ± 92.33 |
|
| 40–59 |
325.8 ± 94.52 |
|
295.46 ± 95.41 |
|
| 60–79 |
341.07 ± 96.24 |
|
315.27 ± 93.68 |
|
| ≥80 |
331.33 ± 115.31 |
|
348.52 ± 83.49 |
|
| Cardiovascular diagnosis |
| 0.143 | | 0.486 |
| No |
327.35 ± 92.67 |
|
311.85 ± 92.09 |
|
| Yes |
340.9 ± 100.01 |
|
304.86 ± 97.72 |
|
| Digestive diagnosis |
| 0.02 | | 0.365 |
| No |
326.66 ± 94.44 |
|
308.19 ± 93.86 |
|
| Yes |
358.45 ± 89.83 |
|
322.45 ± 92.68 |
|
| Neurological diagnosis |
| 0.521 | | 0.034 |
| No |
328.09 ± 96.63 |
|
303.38 ± 97.78 |
|
| Yes |
333.71 ± 90.94 |
|
321.73 ± 84.67 |
|
| Surgical intervention* |
| <0.001 | | 0.004 |
| Non-surgical |
307.88 ± 84.71 |
|
301.87 ± 97.61 |
|
| Programmed |
319.48 ± 95.12 |
|
303.13 ± 63.33 |
|
| Urgent |
374.71 ± 85.14 |
|
337.98 ± 95.85 |
|
| Vasoactive drugs prior to ICU admission |
| <0.001 | | <0.001 |
| No |
308.34 ± 89.14 |
|
293.31 ± 92.44 |
|
| Yes |
363.34 ± 92.6 |
|
342.38 ± 87.83 |
|
| Category TISS 28* |
| <0.001 | | <0.001 |
| II |
155.29 ± 26.72 |
|
154.89 ± 28.83 |
|
| III |
312.85 ± 54.9 |
|
306.97 ± 55.73 |
|
| IV |
451.56 ± 35.28 |
|
446.14 ± 28.37 |
|
ICU – Intensive Care Unit, SD – Standard Deviation,
TISS 28 – Simplified Therapeutic Intervention Score System,
* The Kruskal-Wallis test was applied to these variables, and the Mann-Whitney U test was applied to the other variables.
Another element identified in the results is the direct relationship between workload and negative
patient health outcomes. For the two ICUs compared, the proportion of deaths, adverse events (AEs),
and hospital stays longer than 7 days increased in direct proportion to the patients' TISS-28 category,
meaning that patients with greater care requirements had worse health outcomes (Table 5). The ICU-2
(Auxiliary) showed higher proportions of deaths, AEs, and prolonged stays at TISS-28 levels III and
IV compared to the ICU-1 (Nurses), suggesting that, despite the overload present in both ICUs, the
ICU-1 (Nurses) model provides safer care (Table 5). The proportion of deaths by TISS-28 level and the
care times associated with this variable (Table 4) demonstrate the importance of this instrument as a
predictor of mortality.
Table 5. Comparison of clinical outcomes by TISS-28 category
X
Table 5. Comparison of clinical outcomes by TISS-28 category
| Variable – TISS Levels 28 |
ICU 1 Nurses
% (Yes) |
% (No) |
p-value* |
ICU 2 Assistants
% (Yes) |
% (No) |
p-value* |
| Death |
| | <0.001 |
| | <0.001 |
| II |
0 (0) |
100 (51) |
|
1.61 (1) |
98.38 (61) |
|
| III |
7.14 (26) |
92.85 (338) |
|
11.56 (37) |
88.43 (283) |
|
| IV |
33.33 (42) |
66.66 (84) |
|
49.35 (38) |
50.64 (39) |
|
| Adverse events |
| | <0.001 |
| | <0.001 |
| II |
7.84 (4) |
92.15 (47) |
|
24.19 (15) |
75.80 (47) |
|
| III |
47.80 (174) |
52.19 (190) |
|
59.06 (189) |
40.93 (131) |
|
| IV |
80.16 (101) |
19.84 (25) |
|
92.20 (71) |
7.79 (6) |
|
| Stay >7 days |
| | <0.001 |
| | <0.001 |
| II |
5.88 (3) |
94.11 (48) |
|
3.22 (2) |
96.77 (60) |
|
| III |
24.45 (89) |
75.54 (275) |
|
30.62 (98) |
69.37 (222) |
|
| IV |
46.83 (59) |
53.17 (67) |
|
67.53 (52) |
32.46 (25) |
|
ICU – Intensive Care Unit,
TISS 28 – Simplified Therapeutic Intervention Score System,
* p value for chi square.
Discusión
The analysis of the results will be presented in three levels or layers of analysis. First, the explicit
findings indicated by the data regarding workload, patient characteristics, and nurse characteristics
will be discussed. The second layer of analysis allows for an exploration of implicit aspects related
to the organizational structures of nursing work in the ICU. The third layer proposes a broader level
of considerations that reflect the value of care as a public good, including public policies and the
generation of nursing knowledge. Finally, the limitations of the study will be assessed within the
framework of the analyzed results.
Insufficient nurse allocation in the face of high patient dependency is the main factor generating
work overload in the ICU, a common aspect in this study and in the literature consulted in Colombia
and Latin America
5,
11,
13,
20,
24-
26.
The studies show that, although most patients were classified as TISS-28
levels III and IV, the number of nurses assigned was always below that suggested by the instrument,
with heterogeneous ranges from 1:3 nurses per patient to 1:12.
It is worth noting that none of the studies mentioned indicate that patient allocation within a nursing
team is based on the TISS-28 or any scale based on patient status; that is, the number of patients in the
ward is divided among the number of nurses regardless of care requirements, generally by geography.
Therefore, the TISS-28 would not be used as a criterion for distributing human resources according to
patient severity.
A second point to highlight is that there are few studies that report the distribution of nursing
assistants per patient
11
and that analyze the skill mix in relation to the TISS-28. In our study,
the allocation of nursing assistants to ICU1-Nurses and ICU2-Assistants is appropriate compared to
that estimated by the TISS-28 and coincides with that reported by Arango
11.
The shortage of nurses compared to the sufficiency of nursing assistants reveals how hospital
institutions meet the need for human resources by hiring nursing assistants, because of regulatory gaps
regarding the nurse-to-patient ratio in Colombia. In this regard, it should be noted that the regulations
on minimum operating requirements for hospitals in force in Colombia in 1997
24
established the obligation to assign 1 nurse for every 3 beds and one nursing assistant for every 2, but
in subsequent reforms it was only established that the ICU must have a nurse and a nursing assistant
available without considering the number of beds in operation.
The analysis of activity times in the TISS-28 for nurses and nursing assistants in ICU1-Nurses and ICU2-
Assistants reveals, as do other studies, that most of the care time is dedicated to basic monitoring,
cardiovascular and ventilatory support, and medication administration
26.
The distribution of functions between nursing assistants and nurses in ICU1-Nurses is consistent with
their levels of training and legal responsibility, while in ICU2-Assistants, nursing assistants assume
functions for which they lack the necessary level of competence and legal responsibility, such as the
administration of inotropic and vasoactive medications, invasive airway management, and management
of metabolic complications, to name just a few. The intra-ICU comparison shows that nursing assistants in ICU2-Assistants must
assume a large part of the functions performed exclusively by nurses in ICU1-Nurses.
This phenomenon had already been mentioned by Arango
11
and Ortega and Jiménez
15,
who point out that the role of nurses is concentrated on administrative activities and some limited care,
while nursing assistants are delegated direct care, which includes activities that, due to their level of
knowledge and specialized techniques, are considered non-delegable.
Blay and Roche 27 agree on the same aspects and add the limited supervision of nurses over the work of nursing
assistants. An important factor to consider is that neither nurses nor nursing assistants have influence
over their work environments; that is, they are subject to the logic of delegation imposed by the
institutional ways of organizing nursing work
17.
The discussion presented leads to questioning to what extent the skill The mix of staff, skill level, and
work environments influence patient safety and health outcomes. Data showed that the number of
deaths, adverse events, and length of stay increased directly with the TISS-28 level, meaning that the
increase in these negative outcomes can be explained by workload. Comparing the two ICUs, the
proportion of negative outcomes was lower in the ICU with a higher percentage of nurses in the skill
set. mix, suggesting that their level of qualification allows them to provide safer and higher quality
care. These findings are consistent with studies such as those by Caballero, who reported a high and
inverse correlation between workload and patient safety, presenting a correlation coefficient RHO =
-0.658 and p<0.001
28;
Cho et al.
6
who showed the effects of low staffing, as nurses responsible for the
care of 8 or more patients rated patient safety and quality of care as poor or failing: (OR 5.97, CI 1.33–
26.8, p 0.001) and (OR 5.82, CI 2.91–11.7, p 0.001). Along the same lines, Alrabae et al.
29
established negative correlations between workload and the perception of patient safety culture (r:
-0.721 p < 0.001). Similarly, Aiken et al.
30
demonstrated that overload and the low proportion of professional
nurses in the skill These are factors related to the increase in in-hospital mortality.
The characteristics of patients associated with higher care requirements reported in similar studies are
being male, admission for surgical pathology, experiencing adverse events, death, and hospitalization
longer than 7 days
31-34,26.
These characteristics can guide preventive actions and highlight the
importance of the instrument as a predictor of mortality and as a tool for managing the allocation
and distribution of nursing staff, if its institutional use is adopted.
Regarding the second layer of analysis, it should be considered that one seemingly obvious
consequence of work overload is that nurses are unable to fulfill their assigned tasks and omit
them either partially or completely. From a quantitative perspective, Soliman
35
established direct correlations between workload and omitted care (r = 0.730, p = 0.001). Omitted care was an emerging category in previous research conducted in the same ICUs, where care models were
compared from a qualitative perspective
17.
Staff referred to the workload overload that led them to
prioritize critically ill patients over less critically ill ones, biological interventions over emotional and
family interventions, and to perform tasks less frequently, more quickly, and with lower quality
17.
A complementary perspective on this phenomenon is offered by Mesa and Romero, who point to
the precarious working conditions in which nursing staff carry out their work, characterized by low
wages, unstable employment relationships, and the "jack-of -all-trades" role imposed upon them to
attend to the multiplicity of functions (many of them unrelated to care), which leads them to perform
"care in a rush" or against the clock, which has negative implications for quality
36.
These types of work environments encourage care to be focused on functions and not on people
17.
Regarding the third layer of analysis, it is worth asking: What other realities are hidden behind the
presented data? And what do they suggest in terms of valuing care as a public good? Based on these
questions, this paper aims to analyze some contradictions revealed by the data considering certain
elements of the social organization of care, which together demonstrate an undervaluation of nursing
care as a public good. Menéndez Spina
37
highlights the importance of studying the health-illness-
care-attention processes as "spies" that reveal social contradictions and underscores the contribution
of these contradictions to problematizing reality, offering keys to interpreting the dominant social
order.
The contradictions regarding care are evident when considering that nursing staff constitute
more than 50% of the healthcare workforce, and that in 2018 a campaign called Nursing was carried
out. Now, to highlight and strengthen women's leadership in the health sector, which during the
Covid-19 pandemic saw nurses praised in the media as heroines risking their lives to care for those
affected. However, this contrasts sharply with the fact that in 2024, nursing staff continue to perform
their work with a 39% gender pay gap compared to the medical profession
38,
without recognition of their postgraduate training, under conditions of physical and mental overload,
and their work is being replaced by nursing assistants, who are cheaper for the system but whose work
undermines the quality of care and puts patients' health at risk
15.
At the policy level, it is evident that the regulations of the Colombian health system have not
established a nurse-to-patient ratio; care is conceived as a hotel expense within hospital fee
schedules
39;
and, although there is a National Nursing Policy and a ten-year plan for 2020-2030 that
was developed with the participation of nurses from all over the country, there are few results in
terms of transforming working conditions and generating knowledge to address adverse working
conditions and the contributions of care to patient safety and quality of care. In other words, a policy
instrument exists, but the necessary agency as a political subject that would allow the profession to
advance in transforming its current conditions has not been developed.
Taken together, the arguments presented regarding the microsocial space of workload and the macro
dimension where economic and political forces shape the contexts of care delivery allow us to affirm
that a process of devaluation of nursing care as a public good is underway in Colombian society,
despite its central importance in sustaining and maintaining life. It is primarily the responsibility of
the nursing profession to organize, work, and mobilize to problematize this situation, raise awareness
of it, and seek alternatives for transformation.
Limitations of the study include the implementation timeframe for the pilot study of the two nursing
care models compared (2018-2020), which restricted the data collection period. Furthermore,
research development timelines are limited, especially when part of the research team consists of
nurses working in adult intensive care units, meaning that the knowledge products derived from the
study are generated after the research projects have been concluded.
Conclusion
It was identified that both ICUs have a higher workload for nurses, exceeding the ideal number of
patients proposed by TISS-28, and that their duties are incompatible with the time available per
patient. Some care provided by nursing assistants in ICU-2 does not correspond to their level of training
and legal responsibility, such as administration of medications and vasoactive drugs, ventilatory and
nutritional support, and artificial airway management. Clinical characteristics of the patients, such as
vasoactive drug use prior to ICU admission, transfusions, adverse events, and death, were correlated
with longer care times.
A direct correlation was found between the incidence of adverse events (AEs) , the proportion of
deaths, hospital stays longer than 7 days, and the TISS-28 score in both ICUs, indicating that the nurses
in ICU-1 achieved better results in terms of safety and quality of care. TISS-28 has proven to be a useful
instrument for measuring workload; however, it does not reflect some of the activities performed by
nurses, especially administrative, educational, and socio-emotional tasks. Therefore, future research is
recommended to adapt or create instruments that reflect the complexity of nursing work in the ICU.
Conflict of interest: The authors declare that they have no conflict of interest in the development of
this article.
Funding: This study did not receive funding.
Referencias
X
Referencias
Nasirizad Moghadam K, Chehrzad MM, Reza Masouleh S, Maleki M, Mardani A, Atharyan S, et al.
Nursing physical workload and mental workload in intensive care units: Are they related?
Nurs Open. 2021;8(4):1625–33.
http://dx.doi.org/10.1002/nop2.785
X
Referencias
Schubert M, Ausserhofer D, Bragadóttir H, Rochefort CM, Bruyneel L, Stemmer R, et al.
Interventions to prevent or reduce rationing or missed nursing care: a scoping review.
J Adv Nurs. 2021;77(2):550-564.
https://doi.org/10.1111/jan.14596
X
Referencias
Huaman Julián V, Madueño Delgado A.
Efectividad de la escala TISS 28 para la asignación de pacientes por enfermera en la unidad de cuidados intensivos.
[Tesis Especialista en Enfermería en Cuidados Intensivos] Facultad de ciencias de la salud,
Universidad Privada Norbert Wiener; 2021.
https://repositorio.uwiener.edu.pe/handle/20.500.13053/5881
X
Referencias
Rodríguez Alvira MA, Jiménez Castellanos C, Rodríguez Villarreal HA.
Relación entre carga laboral y calidad del cuidado en pacientes críticos de 3 ciudades, Colombia, 2021
[Tesis de maestría en Cuidado Crítico]. Bogotá: Pontificia Universidad Javeriana, 2022.
http://hdl.handle.net/10554/58278
X
Referencias
Cho SH, Lee JY, You SJ, Song KJ, Hong KJ.
Nurse staffing, nurses prioritization, missed care, quality of nursing care, and nurse outcomes.
Int J Nurs Pract. 2020;26(1):e12803.
https://doi.org/10.1111/ijn.12803
X
Referencias
Schubert M, Ausserhofer D, Bragadóttir H, Rochefort CM, Bruyneel L, Stemmer R, et al.
Interventions to prevent or reduce rationing or missed nursing care: a scoping review.
J Adv Nurs. 2021;77(2):550-564.
https://doi.org/10.1111/jan.14596
X
Referencias
Twigg DE, Whitehead L, Doleman G, El-Zaemey S.
The impact of nurse staffing methodologies on nurse and patient outcomes: A systematic review.
J Adv Nurs. 2021;77(12):4599-4611.
https://doi.org/10.1111/jan.14909
X
Referencias
Soliman MS, Eldeep NM.
The relationship among workload, teamwork, and missed nursing care at intensive care units.
Egypt J Health Care. 2020;11(3):603-611.
https://doi.org/10.21608/ejhc.2020.163259
X
Referencias
Pereira Lima Silva R, Gonçalves Menegueti M, Dias Castilho Siqueira L, de Araújo TR,
Auxiliadora-Martins M, Mantovani Silva Andrade L, et al.
Omission of nursing care, professional practice environment and workload in intensive care units.
J Nurs Manag. 2020;28(8):1986-1996.
https://doi.org/10.1111/jonm.13005
X
Referencias
Arango GL, Peña B, Vega Y.
Relación de la asignación de personal de enfermería con indicadores
de resultado de la calidad de la atención en unidades de cuidados intensivos de adultos.
Aquichán. 2015;15(1):90-104.
https://doi.org/10.5294/aqui.2015.15.1.9
X
Referencias
Romero-Massa E, Lorduy-Bolívar JP, Pájaro-Melgar C, Pérez-Duque CA.
Relación entre la carga laboral de enfermería y la gravedad del paciente en unidades de cuidado intensivo de adultos.
Aquichan. 2011;11(2):173-186.
https://doi.org/10.5294/aqui.2011.11.2.4
X
Referencias
Achury Saldaña DM, Achury Beltrán LF, Díaz Alvarez JC, Rodríguez Colmenares SM, Alvarado
HR, Ortiz C, et al.
Panorama general de la relación enfermera-paciente en algunas unidades
de cuidado intensivo en Bogotá.
Investig Enferm Imagen Desarr. 2014;16(1):73-85.
https://doi.org/10.11144/Javeriana.IE16-1.pgre
X
Referencias
López Cárdenas WI, Henao Murillo NA, Gil Vidal E, Altamirano Ceron RM, Santa Mejía YA,
Jurado Jiménez AC.
Percepciones de atención en dos modelos de prestación de atención de
enfermería en UCI: un enfoque cualitativo-comparativo.
Investigación y Educación en Enfermería. 2023;40(3).
https://doi.org/10.17533/udea.iee.v40n3e15
X
Referencias
Gil Vidal E.
Retrasar u omitir el cuidado de enfermería: la experiencia de enfermeras de Unidades de
Cuidado Intensivo en Medellín, 2020-2023
[Tesis de maestría en Enfermería] Medellín, Colombia,
Universidad de Antioquia; 2023.
https://hdl.handle.net/10495/40053
X
Referencias
Escobar Bermúdez A, Martínez Ceballos JF, Montenegro Rangel LP, Vargas Zúñiga ML, Arias
Torres D.
Nurse-patient relationship according to TISS 28. Clinical application at Intensive Care
Unit – 2011.
RFS. 2012;4(2):55-6.
https://doi.org/10.25054/rfs.v4i2.98
X
Referencias
Moghadam KN, Chehrzad MM, Masouleh SR, Mardani A, Maleki M, Akhlaghi E, et al.
Nursing workload in intensive care units and the influence of patient and nurse characteristics.
Nurs Crit Care. 2021;26(6):425-431.
https://doi.org/10.1111/nicc.12548
X
Referencias
Alarcón-Chávez MCDLL, Flores-Padilla MJB, Gómez-Jurado MIBC.
Análisis de la distribución del tiempo en materia de cuidado crítico por profesionales de enfermería mediante TISS-28.
Univ Nac Auton Mex. [Internet]. 2020 [citado 2024 Feb 10];1–11.
Disponible en:
https://repositorio.unam.mx/contenidos/4128645
X
Referencias
Pérez Gutiérrez N, Rodríguez Darabos EI.
Talento humano en unidades de cuidado intensivo:
adaptación de un modelo de estándares para Colombia basado en la evidencia científica.
Acta Colombiana de Cuid Intens. 2015;15(2):80-102.
https://doi.org/10.1016/j.acci.2015.02.006
X
Referencias
Simões JL, Sa-Couto P, Simões CJ, Oliveira C, Dos Santos NM, Mateus J, et al.
Nursing workload assessment in an intensive care unit: A 5-year retrospective analysis.
J Clin Nurs. 2021;30(3-4):528-40.
https://doi.org/10.1111/jocn.15570
X
Referencias
Blay N, Roche MA.
A systematic review of activities undertaken by the unregulated Nursing Assistant.
J Adv Nurs. 2020;76(7):1538-51.
https://doi.org/10.1111/jan.14354
X
Referencias
Caballero Ramirez MJ.
Sobrecarga laboral y seguridad del paciente en la unidad de cuidados
intensivos de un hospital de Lima, 2023
[Tesis de maestría en gestión de los servicios de salud]
Lima-Perú: Universidad César Vallejo; 2023.
https://hdl.handle.net/20.500.12692/121480
X
Referencias
Alrabae YMA, Aboshaiqah AE, Tumala RB.
The association between self-reported workload and
perceptions of patient safety culture: A study of intensive care unit nurses.
J Clin Nurs. 2021;30(7-8):1003-1017.
https://doi.org/10.1111/jocn.15646
X
Referencias
Aiken LH, Sloane DM, Bruyneel L, Van den Heede K, Griffiths P, Busse R, et al.
Nurse staffing and education and hospital mortality in nine European countries:
a retrospective observational study.
Lancet. 2014;383(9931):1824-1830.
https://doi.org/10.1016/S0140-6736(13)62631-8
X
Referencias
Padilha KG, Sousa RMC, Kimura M, Miyadahira AMK, da Cruz DALM, Vattimo MdeF, et al.
Nursing workload in intensive care units: a study using the Therapeutic Intervention Scoring
System-28 (TISS-28).
Intensive Crit Care Nurs. 2007;23(3):162-9.
https://doi.org/10.1016/j.iccn.2006.07.004
X
Referencias
Garcia PC, Gonçalves LA, Ducci AJ, Toffoleto MC, Ribeiro SC, Padilha KG.
Intervenções terapêuticas em Unidade de Terapia Intensiva: análise segundo o Therapeutic Intervention
Scoring System-28 (TISS-28).
Rev Bras Enfer. 2005;58(2):194–199.
https://doi.org/10.1590/S0034-71672005000200013
X
Referencias
Cáceres Rivera DI, Torres C, Cristancho Zambrano LY, López Romero LA.
Carga laboral de los profesionales de enfermería en unidad de cuidados intensivos:
estudio descriptivo: «CARETIME».
Acta Colomb Cuid Intensivo. 2020;20(2):92-7.
https://doi.org/10.1016/j.acci.2019.12.002
X
Referencias
Soliman SM, Eldeep NM.
La relación entre la carga de trabajo, el trabajo en equipo y los cuidados
de enfermería perdidos en las unidades de cuidados intensivos.
Egypt J Health Care. 2020;11(3):603-11.
https://doi.org/10.21608/ejhc.2020.163259
X
Referencias
Menéndez Spina EL.
Las enfermedades como problematizadoras de la realidad.
Movimientos étnicos, pluralismo asistencial, intelectuales y el «buen vivir».
En: Cuadrada Majó C, editor.
Pluralismo médico y curas alternativas; 2020. p. 51-132.
https://dialnet.unirioja.es/metricas/documentos/ARTLIB/7494077
Alghamdi MG. Nursing workload: a concept analysis. J Nurs Manag. 2016;24(4):449-57. https://doi.org/10.1111/jonm.12354
Nasirizad Moghadam K, Chehrzad MM, Reza Masouleh S, Maleki M, Mardani A, Atharyan S, et al. Nursing physical workload and mental workload in intensive care units: Are they related? Nurs Open. 2021;8(4):1625–33. http://dx.doi.org/10.1002/nop2.785
Schubert M, Ausserhofer D, Bragadóttir H, Rochefort CM, Bruyneel L, Stemmer R, et al. Interventions to prevent or reduce rationing or missed nursing care: a scoping review. J Adv Nurs. 2021;77(2):550-564. https://doi.org/10.1111/jan.14596
Huaman Julián V, Madueño Delgado A. Efectividad de la escala TISS 28 para la asignación de pacientes por enfermera en la unidad de cuidados intensivos. [Tesis Especialista en Enfermería en Cuidados Intensivos]. Facultad de ciencias de la salud, Universidad Privada Norbert Wiener; 2021. https://repositorio.uwiener.edu.pe/handle/20.500.13053/5881
Rodríguez Alvira MA, Jiménez Castellanos C, Rodríguez Villarreal HA. Relación entre carga laboral y calidad del cuidado en pacientes críticos de 3 ciudades, Colombia, 2021. [Tesis de maestría en Cuidado Crítico]. Bogotá: Pontificia Universidad Javeriana; 2022. http://hdl.handle.net/10554/58278
Cho SH, Lee JY, You SJ, Song KJ, Hong KJ. Nurse staffing, nurses prioritization, missed care, quality of nursing care, and nurse outcomes. Int J Nurs Pract. 2020;26(1):e12803. https://doi.org/10.1111/ijn.12803
Schubert M, Ausserhofer D, Bragadóttir H, Rochefort CM, Bruyneel L, Stemmer R, et al. Interventions to prevent or reduce rationing or missed nursing care: a scoping review. J Adv Nurs. 2021;77(2):550-564. https://doi.org/10.1111/jan.14596
Twigg DE, Whitehead L, Doleman G, El-Zaemey S. The impact of nurse staffing methodologies on nurse and patient outcomes: A systematic review. J Adv Nurs. 2021;77(12):4599-4611. https://doi.org/10.1111/jan.14909
Soliman MS, Eldeep NM. The relationship among workload, teamwork, and missed nursing care at intensive care units. Egypt J Health Care. 2020;11(3):603-611. https://doi.org/10.21608/ejhc.2020.163259
Pereira Lima Silva R, Gonçalves Menegueti M, Dias Castilho Siqueira L, de Araújo TR, Auxiliadora-Martins M, Mantovani Silva Andrade L, et al. Omission of nursing care, professional practice environment and workload in intensive care units. J Nurs Manag. 2020;28(8):1986-1996. https://doi.org/10.1111/jonm.13005
Arango GL, Peña B, Vega Y. Relación de la asignación de personal de enfermería con indicadores de resultado de la calidad de la atención en unidades de cuidados intensivos de adultos. Aquichán. 2015;15(1):90-104. https://doi.org/10.5294/aqui.2015.15.1.9
Romero-Massa E, Lorduy-Bolívar JP, Pájaro-Melgar C, Pérez-Duque CA. Relación entre la carga laboral de enfermería y la gravedad del paciente en unidades de cuidado intensivo de adultos. Aquichan. 2011;11(2):173-186. https://doi.org/10.5294/aqui.2011.11.2.4
Cogollo Hernández J, Navarro Vélez PA. Medición de las alteraciones de salud de los usuarios y su relación con la asignación del personal de enfermería de una UCI de la ciudad de Montería, Colombia, 2022. [Tesis Especialización en auditoría de la calidad en salud]. Montería: Facultad Ciencias de la Salud, Universidad de Córdoba; 2022. https://repositorio.unicordoba.edu.co/server/api/core/bitstreams/0de7bf13-27fb-4ad7-86b1-e7f04c0a715e/content
Achury Saldaña DM, Achury Beltrán LF, Díaz Alvarez JC, Rodríguez Colmenares SM, Alvarado HR, Ortiz C, et al. Panorama general de la relación enfermera-paciente en algunas unidades de cuidado intensivo en Bogotá. Investig Enferm Imagen Desarr. 2014;16(1):73-85. https://doi.org/10.11144/Javeriana.IE16-1.pgre
Ortega M, Jiménez A. Situación actual de enfermería en Colombia: una reflexión. Rev Ocup Humana. 2020;9(1):28-38. https://revistas.unipamplona.edu.co/ojs_viceinves/index.php/COH/article/view/4448/0
Asociación Colombiana de Estudiantes de Enfermería (ACOEEN). Política Nacional de Enfermería 2020-2030 - ACOEEN [Internet]. Org.co. 2020 [citado 2023 Feb 6]. https://www.acoeen.org.co/index.php/eventos/politica-nacional-de-enfermeria-2020-2030
López Cárdenas WI, Henao Murillo NA, Gil Vidal E, Altamirano Ceron RM, Santa Mejía YA, Jurado Jiménez AC. Percepciones de atención en dos modelos de prestación de atención de enfermería en UCI: un enfoque cualitativo-comparativo. Investigación y Educación en Enfermería. 2023;40(3). https://doi.org/10.17533/udea.iee.v40n3e15
Gil Vidal E. Retrasar u omitir el cuidado de enfermería: la experiencia de enfermeras de Unidades de Cuidado Intensivo en Medellín, 2020-2023. [Tesis de maestría en Enfermería]. Medellín, Colombia: Universidad de Antioquia; 2023. https://hdl.handle.net/10495/40053
Rivera DIC, Torres CC, Romero LAL. Factors associated with nursing workload in three intensive care units. Rev Esc Enferm USP. 2021;55:e20200272. https://doi.org/10.1590/1980-220X-REEUSP-2020-0272
Escobar Bermúdez A, Martínez Ceballos JF, Montenegro Rangel LP, Vargas Zúñiga ML, Arias Torres D. Nurse-patient relationship according to TISS 28. Clinical application at Intensive Care Unit – 2011. RFS. 2012;4(2):55-6. https://doi.org/10.25054/rfs.v4i2.98
Moghadam KN, Chehrzad MM, Masouleh SR, Mardani A, Maleki M, Akhlaghi E, et al. Nursing workload in intensive care units and the influence of patient and nurse characteristics. Nurs Crit Care. 2021;26(6):425-431. https://doi.org/10.1111/nicc.12548
Alarcón-Chávez MCDLL, Flores-Padilla MJB, Gómez-Jurado MIBC. Análisis de la distribución del tiempo en materia de cuidado crítico por profesionales de enfermería mediante TISS-28. Univ Nac Auton Mex. [Internet]. 2020 [citado 2024 Feb 10];1–11. https://repositorio.unam.mx/contenidos/4128645
López Cárdenas WI. Cuidado de enfermería-desenlaces en UCI adultos. Mendeley Data V1. 2025. https://doi.org/10.17632/gnhz6g9vmh.1
Acosta Nuñez JM, Sandoval Balarezo GM, Paredes Garcés MG, Supe Supe FA. Carga laboral en áreas críticas y “TISS 28”. Salud, Cienc Tecnol. 2023;3:385. https://doi.org/10.56294/saludcyt2023385
Pérez Gutiérrez N, Rodríguez Darabos EI. Talento humano en unidades de cuidado intensivo: adaptación de un modelo de estándares para Colombia basado en la evidencia científica. Acta Colombiana de Cuid Intens. 2015;15(2):80-102. https://doi.org/10.1016/j.acci.2015.02.006
Simões JL, Sa-Couto P, Simões CJ, Oliveira C, Dos Santos NM, Mateus J, et al. Nursing workload assessment in an intensive care unit: A 5-year retrospective analysis. J Clin Nurs. 2021;30(3-4):528-40. https://doi.org/10.1111/jocn.15570
Blay N, Roche MA. A systematic review of activities undertaken by the unregulated Nursing Assistant. J Adv Nurs. 2020;76(7):1538-51. https://doi.org/10.1111/jan.14354
Caballero Ramirez MJ. Sobrecarga laboral y seguridad del paciente en la unidad de cuidados intensivos de un hospital de Lima, 2023. [Tesis de maestría en gestión de los servicios de salud]. Lima-Perú: Universidad César Vallejo; 2023. https://hdl.handle.net/20.500.12692/121480
Alrabae YMA, Aboshaiqah AE, Tumala RB. The association between self-reported workload and perceptions of patient safety culture: A study of intensive care unit nurses. J Clin Nurs. 2021;30(7-8):1003-1017. https://doi.org/10.1111/jocn.15646
Aiken LH, Sloane DM, Bruyneel L, Van den Heede K, Griffiths P, Busse R, et al. Nurse staffing and education and hospital mortality in nine European countries: a retrospective observational study. Lancet. 2014;383(9931):1824-1830. https://doi.org/10.1016/S0140-6736(13)62631-8
Padilha KG, Sousa RMC, Kimura M, Miyadahira AMK, da Cruz DALM, Vattimo MdeF, et al. Nursing workload in intensive care units: a study using the Therapeutic Intervention Scoring System-28 (TISS-28). Intensive Crit Care Nurs. 2007;23(3):162-9. https://doi.org/10.1016/j.iccn.2006.07.004
Balsanelli AP, Zanei SSSV, Whitaker IY. Carga de trabalho de enfermagem e sua relação com a gravidade dos pacientes cirúrgicos em UTI. Acta Paul Enferm. 2006;19(1):16-20. https://doi.org/10.1590/S0103-21002006000100003
Garcia PC, Gonçalves LA, Ducci AJ, Toffoleto MC, Ribeiro SC, Padilha KG. Intervenções terapêuticas em Unidade de Terapia Intensiva: análise segundo o Therapeutic Intervention Scoring System-28 (TISS-28). Rev Bras Enfer. 2005;58(2):194–199. https://doi.org/10.1590/S0034-71672005000200013
Cáceres Rivera DI, Torres C, Cristancho Zambrano LY, López Romero LA. Carga laboral de los profesionales de enfermería en unidad de cuidados intensivos: estudio descriptivo: «CARETIME». Acta Colomb Cuid Intensivo. 2020;20(2):92-7. https://doi.org/10.1016/j.acci.2019.12.002
Soliman SM, Eldeep NM. La relación entre la carga de trabajo, el trabajo en equipo y los cuidados de enfermería perdidos en las unidades de cuidados intensivos. Egypt J Health Care. 2020;11(3):603-11. https://doi.org/10.21608/ejhc.2020.163259
Mesa Melgarejo L, Romero Ballén MN. Profesionales de enfermería y cuidado en las condiciones laborales actuales. Investig Enferm Imagen Desarrol. 2010;12(2):55-92. https://www.redalyc.org/pdf/1452/145217280005.pdf
Menéndez Spina EL. Las enfermedades como problematizadoras de la realidad. Movimientos étnicos, pluralismo asistencial, intelectuales y el «buen vivir». En: Cuadrada Majó C, editor. Pluralismo médico y curas alternativas; 2020. p. 51-132. https://dialnet.unirioja.es/metricas/documentos/ARTLIB/7494077
Cuestión pública. Con o sin COVID-19: Colombia es mala paga para las mujeres en la salud. [Internet]. 2020 Sep 24 [citado 2024 Feb 20]. https://cuestionpublica.com/desigualdad-salarial-de-genero-en-sector-salud-colombia/colombia-es-mala-paga-para-las-mujeres-en-la-salud/
Ministerio de Salud y Protección Social. Decreto 2423 de 1996. Consulta: Feb 20, 2024. https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/DE/DIJ/decreto-2423-de-1996.pdf