Rev Cuid. 2026; 17(1): 4585
Abstract
Introduction: With the increasing aging of the population, nursing training must address disability profiles in adults. Objective: To identify whether Nursing Interventions Classification (NIC) with a population over 29 years of age, carried out by a University Program during intramural practices in hospital institutions, respond to health care guidelines for healthy aging in Colombia. Materials and Methods: A quantitative cross-sectional descriptive study with an analytical component. Purposive sampling was used. A database containing 13,368 NIC records performed between 2021 and 2023 that met inclusion criteria was analyzed. The population served was characterized; intervention frequencies were obtained according to Functional Health Patterns (FHPs). Using an 80% discrimination standard, five FHPs were included, covering 87.6% (11,714) of the records. Diagnoses and interventions were identified by domains and interpreted according to Colombia's Aging Policy. SPSS-v.26 was used. Results: The population between 29 and 98 years old was attended, with similar proportions between adults: 50.47% (1,225) and older adults: 49.63% (1,206); male predominance: 62.42% (1,517). The highlighted PFS were Activity and exercise: 33.12% (4,428) and Nutritional-metabolic: 24.17% (2,830), and NIC predominated in the complex physiological domain: 39.29% (4,603): medication administration 48.97% (2,254) and in the basic physiological domain 25.99% (3,045): elimination management 24.86% (757). Discussion: Interventions are aligned with the goals of wellness, quality of life and autonomy for healthy aging. Conclusions: The University Institution fulfills its function of training Nursing professionals who respond to the needs of the social environment framed by Public Policies.
Keywords: Education Nursing; Standardized Nursing Terminology; Professional Training; Adult Health; Healthy Aging.
Resumen
Introducción: Con el creciente envejecimiento de la población, la formación de enfermeros debe abordar perfiles de discapacidad en adultos. Objetivo: Identificar si las intervenciones de Enfermería (NIC) con población mayor de 29 años, realizadas por un programa universitario durante las prácticas intramurales en instituciones hospitalarias, responden a las directrices de atención en salud para el envejecimiento saludable en Colombia. Materiales y Métodos: Estudio descriptivo transversal cuantitativo, con componente analítico. Muestreo intencional. Se analizó una base de datos con 13.368 registros de NIC realizadas entre 2021 y 2023, que cumplieron criterios de inclusión. Se caracterizó la población atendida; se obtuvieron frecuencias de Intervenciones según Patrones Funcionales de Salud (PFS). Con pauta de discriminación del 80% quedaron incluidos cinco PFS abarcando el 87,6% (11.714) de los registros; se identificaron diagnósticos e intervenciones por Dominios que se interpretaron según Política de Envejecimiento en Colombia. Se utilizó SPSS-v.26. Resultados: Se atendió población entre 29 y 98 años, con proporciones similares entre adultos: 50,47% (1.225) y adultos mayores: 49,63% (1.206); predominio masculino: 62,42% (1.517). Los PFS destacados fueron Actividad y ejercicio: 33,12% (4.428) y Nutricional-metabólico: 24,17% (2.830) y, predominaron NIC en dominio fisiológico complejo: 39,29% (4.603): administración de medicación 48,97% (2.254) y en dominio fisiológico básico 25,99% (3.045): manejo de eliminación 24,86% (757). Discusión: Las intervenciones se alinean con las metas de bienestar, calidad de vida y autonomía para un envejecimiento saludable. Conclusiones: La Institución Universitaria cumple su función de formar profesionales de Enfermería que responden a necesidades del medio social enmarcadas en Políticas Públicas.
Palabras Clave: Educación en Enfermería; Terminología Normalizada de Enfermería; Formación Profesional; Salud del Adulto; Envejecimiento Saludable.
Resumo
Introdução: Com o crescente envelhecimento da população, a formação em enfermagem deve abordar os perfis de incapacidade em adultos. Objetivo: Identificar se as intervenções de Enfermagem (NIC) com uma população acima de 29 anos, realizadas por um programa universitário durante práticas de internação em instituições hospitalares, atendem às diretrizes de saúde para o envelhecimento saudável na Colômbia. Materiais e Métodos: Estudo quantitativo, transversal, descritivo, com componente analítico. Amostragem intencional. Foi analisado um banco de dados com 13.368 registros de NIC realizados entre 2021 e 2023 que atenderam aos critérios de inclusão. A população atendida foi caracterizada; as frequências das intervenções foram obtidas de acordo com os Padrões Funcionais de Saúde (PSF). Utilizando um padrão de discriminação de 80%, cinco PSF foram incluídos, abrangendo 87,6% (11.714) dos registros. Diagnósticos e intervenções foram identificados por Domínios, que foram interpretados de acordo com a Política do Envelhecimento na Colômbia. Utilizou-se o SPSS-v.26. Resultados: Foi atendida a população entre 29 e 98 anos, com proporções semelhantes entre adultos: 50,47% (1.225) e idosos: 49,63% (1.206); predomínio do sexo masculino: 62,42% (1.517). As EFP destacadas foram Atividade e exercício: 33,12% (4.428) e Nutricional-metabólica: 24,17% (2.830), sendo que a NIC predominou no domínio fisiológico complexo: 39,29% (4.603): administração de medicamentos 48,97% (2.254) e no domínio fisiológico básico 25,99% (3.045): manejo da eliminação 24,86% (757). Discussão: As intervenções estão alinhadas aos objetivos de bem-estar, qualidade de vida e autonomia para um envelhecimento saudável. Conclusões: A Instituição Universitária cumpre sua função de formar profissionais de Enfermagem que respondam às necessidades do meio social enquadradas pelas Políticas Públicas.
Palavras-Chave: Educação em Enfermagem; Terminologia Padronizada em Enfermagem; Formação Profissional; Saúde do Adulto; Envelhecimento Saudável.
Introduction
In 2022, the World Health Organization (WHO) predicted that by 2050, the proportion of people over 60 years of age globally will double, from 12% to 22%, and 80% of these people will live in low- and middle-income countries. Considering that aging directly affects the well-being of older adults, countries must respond with care and social assistance models according to the rate of population aging and the progressive increase in years lived with disability, among the population aged 80 and over1,2. The WHO proposes the Decade of Healthy Aging (2021-2030) and in its Action Plan calls for the economic, social, political, educational and cultural commitment of all people seeking independence and autonomy for older adults3.
Colombia, like the rest of the world, is an aging country. The population over 60 years old increased from 7.5% in 1995 to 15.2% in 2024. The departments with the highest proportion of older people are Quindío: 19.7%, Caldas: 19.3% and Risaralda: 18.4%. These departments have the highest dependency rates for people over 60 years old: Quindío: 31.72%, Caldas: 31.44% and Risaralda, 29.80%4. Changes in population structure and the resulting regulations require healthcare training institutions to understand the social phenomena involved and anticipate short- and medium-term challenges in providing care to adults and older adults.
In defense of the protection of Human Rights of Older Persons, Colombia ratified the provisions of the Inter-American Convention of the Organization of American States (OAS) in June 20155, decreed the Ten-Year Public Health Plan 2022-2031 which included the goal of promoting the functional capacity of the population over 60 years of age6. ALikewise, with Decree 681 of 20227 The National Public Policy on Aging and Old Age 2022-2031 was adopted. Currently in Colombia, aging is seen as a fundamental right, as the right to life and dignity in old age; its attention should emphasize the promotion and social protection for care and social assistance, impacting quality of life and well- being8. Among the strategies for Comprehensive Health Care with a differential approach is the Promotion and Protection of Older Persons from the Comprehensive Care Route for the Promotion and Maintenance of Health9.
These guidelines aim to ensure healthy aging, a dignified, autonomous, and independent old age. Current evidence highlights the importance of nursing's role in active and healthy aging policies and emphasizes the need to adopt a comprehensive, life-course perspective in nursing education. professional10.
Nurses, as providers of care and health educators par excellence, learn during their training about the care of older people with chronic conditions and progressive deterioration that require long- term management and continuous care; it is precisely in these situations when the rigorous implementation of the Nursing Process becomes crucial, becoming a fundamental tool in the development of competencies for the comprehensive and integrated care of human needs at both the individual and collective levels11. The use of the Nursing Process in professional training using standardized language allows for the administration of individualized and patient-centered care while ensuring continuity and consistency of care, favors the teaching-learning process and integra- tes the development of critical and reflective thinking12.
The NANDA (North American Nursing Diagnosis Association)-NOC (Nursing Outcomes Classifica- tion)-NIC taxonomy has been standardized internationally. NANDA International Taxonomy II (NANDA-I) categorizes nursing diagnoses into domains and classes, and the latest edition (13th ed.).
NANDA-I 2024–2026, uses Marjory Gordon 's Functional Health Patterns (FHPs)13. This manuscript will use the term “Functional Health Patterns” (FHP) and seeks to draw attention to the functional dimensions that structure the comprehensive assessment of the human being, without personalizing the approach with emphasis on the author. The classification of nursing interventions with the NIC taxonomy seeks the standardization and systematization of care in its 8th Edition (2024), the NIC taxonomy has registered 610 intervention labels that are grouped into 7 Domains: 1: Basic Physiological, 2: Complex Physiological, 3: Behavioral, 4: Safety, 5: Family, 6: Health system and 7: Community14.
Authors propose that the effective integration of NIC in the training of Nurses is emerging as a fundamental pillar for the development of competent, committed and trained professionals for psychosocial care15-16, hence, at the University Foundation of the Andean Area-Colombia, since 2011, the Training Practices Information System F_PAE was created and registered nationally, which includes variables of the population served, Teaching-Service Relationship and Nursing Care Processes. This software was created with the NANDA-NOC-NIC taxonomy and is fed by the permanent record of care activities of students and teachers. This study analyzes the Nursing Interventions (NIC) conducted between 2021 and 2023 in the population over 29 years of age during hospital practices of a university program, to evaluate their alignment with the Colombian guidelines for healthy aging. The outcomes will explore how students integrate diagnoses, interventions, and learning with social needs and demographic changes17, with the goal of preparing future nurses to face the challenges of chronic disease prevention and comprehensive care for hospitalized adults and older adults, thus contributing to improving the quality of life of these population groups.
Materials and Methods
A descriptive, cross-sectional, quantitative study with an analytical component was conducted, based on the secondary analysis of data from the F_PAE institutional system (F_PAE1361245/30-06- 2017)18, registered with the Ministry of the Interior of Colombia. This system, developed by the Andean Area University Foundation, collects information on the service of the population, the teaching-service relationship, and nursing care processes during students' clinical practices.
Population and sample
Of a total of 28,664 records corresponding to the 2021-2023 period, 13,368 records were intentionally selected that met the following inclusion criteria: (1) complete and correctly completed registration; (2) individuals in the adult and old age life courses (≥29 years); (3) interventions carried out in hospital institutions within the framework of teaching-service agreements. Records from the community area were excluded due to underreporting caused by health restrictions during the COVID-19 pandemic.
Ethical considerations
The Ethics Committee of the Andean Area University Foundation (Minutes of July 27, 2022) approved the study. Access to the database was exclusive to the research team. All records were anonymized and coded to preserve confidentiality.
Variables and data analysis
The population was characterized by age, sex, insurance status, socioeconomic status, and type of clinical practice. The relationships between sociodemographic variables and functional health patterns (FHP) were explored using the chi-square test, with a statistical significance level of p < 0.05. IBM SPSS Statistics v.26 software was used for the analysis.
For the analysis of nursing interventions, frequencies were identified by PFS. An 80% discrimination standard was applied to ensure that the categories represent consistent and statistically relevant patterns within the sample, aligning with quantitative standards of representativeness and validity19, selecting five PFS that concentrated 87.6% (n=11,714) of the total records. In each PFS, the prevalent nursing diagnoses were determined, and the interventions were classified according to the seven domains established by the NIC taxonomy (8th edition, 2024).
The results were interpreted considering the National Policy on Aging and Old Age, allowing for an assessment of the correspondence between the interventions implemented and the guidelines for healthy aging. The complete data set analyzed is available in open access through the Papyrus Dataset repository20.
Results
Sociodemographic characteristics
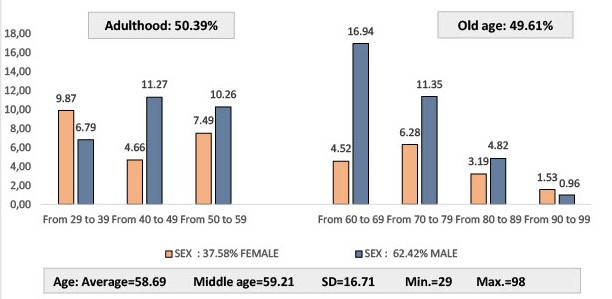
From 2021 to 2023, during the internships carried out by students of the Areandina Nursing Program in different health institutions, 13,368 NIC interventions were recorded in the Institutional Information System on 2,431 people aged 29 and over. As can be seen in Figure 1, the proportion of people by life course was similar: Adulthood: 50.37 % (1,225) and Old Age: 49.63 % (1,206). While among adults (up to 64 years of age) the female population between 30 and 39 years old predominated, in older adults the proportion of the male population was higher, mainly in the 60 to 69 age group.
Regarding health insurance, the largest proportion of the population corresponded to the subsidized regime: 64.93% (1,579). People living in strata 1, 2, and 3 accounted for 97.12% (12,983) of the total study population. The types of practices that recorded the highest proportions of people served were Scientific Principles of Care: 57.09% (1,388), Nursing Care for Adults and Families I: 20.61% (501), and Nursing Care for Adults and Families II: 14.22% (346); the remainder: 8.10% (197) corresponded to other healthcare practices. Table 1 presents the significant relationships between sociodemographic variables and all PFS.
Table 1. Significant relationships between Functional Health Patterns and sociodemographic variables of the adult and elderly population served.
X
Table 1. Significant relationships between Functional Health Patterns and sociodemographic variables of the adult and elderly population served.
| Functional Health Pattern |
Sociodemographic Characteristics |
p-value |
Chi square |
| PFS.1-Perception of Health Maintenance |
Sex |
0.001 |
26.18 |
| PFS.1-Perception of Health Maintenance |
Social security system |
0.001 |
43.17 |
| PFS.1-Perception of Health Maintenance |
SE housing stratum |
0.001 |
87.14 |
| PPFS.1-Perception of Health Maintenance |
Age Group |
0.001 |
101.24 |
| PFS.2-Nutritional - metabolic |
Sex |
0.001 |
105.38 |
| PFS.2-Nutritional - metabolic |
Age Group |
0.001 |
489.13 |
| PFS.3-Elimination |
Sex |
0.001 |
338.17 |
| PFS.3-Elimination |
SE housing stratum |
0.001 |
100.89 |
| PFS.3-Elimination |
Age Group |
0.001 |
1423.96 |
| PFS.4 Activity - exercise |
Social security system |
0.001 |
46.56 |
| PFS.4 Activity - exercise |
Age Group |
0.001 |
341.84 |
| PFS.5 Rest - Sleep |
Social security system |
0.017 |
8.16 |
| PFS.5 Rest - Sleep |
SE housing stratum |
0.010 |
14.99 |
| PFS.5 Rest - Sleep |
Age Group |
0.001 |
44.02 |
| PFS.6 Cognitive perceptual |
Social security system |
0.028 |
7.17 |
| PFS.6 Cognitive perceptual |
Sex |
0.001 |
26.40 |
| PFS.6 Cognitive perceptual |
SE housing stratum |
0.001 |
21.69 |
| PFS.6 Cognitive perceptual |
Age Group |
0.001 |
114.69 |
| PFS.7 Self-image - Self-concept |
Social security system |
0.001 |
77.97 |
| PFS.7 Self-image - Self-concept |
SE housing stratum |
0.001 |
24.18 |
| PFS.7 Self-image - Self-concept |
Age Group |
0.001 |
116.63 |
| PFS.8 Role Relationships |
Social security system |
0.001 |
40.30 |
| PFS.8 Role Relationships |
SE housing stratum |
0.001 |
37.87 |
| PFS.8 Role Relationships |
Age Group |
0.001 |
53.09 |
| PFS.9 Sexuality - Reproduction |
Sex |
0.001 |
67.29 |
| PFS.9 Sexuality - Reproduction |
SE housing stratum |
0.001 |
40.03 |
| PFS.9 Sexuality - Reproduction |
Age Group |
0.001 |
162.62 |
| PFS.10 Coping - Stress Tolerance |
Sex |
0.001 |
11.85 |
| PFS.10 Coping - Stress Tolerance |
Social security system |
0.010 |
9.29 |
| PFS.10 Coping - Stress Tolerance |
Age Group |
0.001 |
152.84 |
| PFS.11 Values - Beliefs |
Social security system |
0.002 |
12.97 |
| PFS.11 Values - Beliefs |
SE housing stratum |
0.001 |
68.85 |
| PFS.11 Values - Beliefs |
Age Group |
0.003 |
21.28 |
Sources: Nursing Training Practice Information System. Andean Area University Foundation - Pereira and author calculation
As can be seen, the sociodemographic variables: age group (adulthood or old age), sex (female or male), health insurance regime (contributory or subsidized) and housing stratum (low-medium) significantly influence the impact of functional patterns in the population analyzed.
Distribution of Functional Health Patterns
A predominance of five patterns was observed, which covered 87.60% (11,714) of the interventions: Activity/exercise: 33.12% (4,428), Nutritional metabolic: 21.17% (2,830), Elimination: 16.15% (2,159), Perception Health Management: 9.45% (1,263) and Cognitive/perceptive: 7.73% (1,034). In the six remaining PFS only 12.37% (1,654) of the total interventions were recorded.
Table 2 relates some characteristics of the population served to the relevant PFS. For all PFS, it was common to find that most patients were male, from Risaralda, living in low-income housing, and served by the subsidized health system.
Table 2. Relevant functional health patterns according to the characteristics of the population served
X
Table 2. Relevant functional health patterns according to the characteristics of the population served
| Characteristics |
Functional Health Patterns |
| PFS4 Activity/Exercise % (n=815) |
PFS2 Nutritional Metabolic % (n=515) |
PFS3 Elimination % (n=393) |
PFS1 Perception Management Health % (n=230) |
PFS6 Cognitive/ perceptual % (n=188) |
Rest of PFS % (n=301) |
| Life course |
|
|
|
|
|
|
| Adulthood |
47.02 (378) |
64.95 (334) |
30.25 (119) |
40.30 (93) |
60.64 (114) |
62.05 (187) |
| Old age |
52.98 (427) |
35.05 (181) |
69.75 (274) |
59.70 (137) |
39.36 (74) |
37.95 (114) |
| Age group |
|
|
|
|
|
|
| From 29 a 39 |
13.37 (108) |
28.23 (145) |
6.76 (27) |
16.39 (38) |
14.89 (28) |
19.96 (60) |
| From 40 a 49 |
15.22 (123) |
17.17 (88) |
7.92 (31) |
12.27 (28) |
24.08 (45) |
23.85 (72) |
| From 50 a 59 |
18.43 (148) |
19.54 (101) |
15.56 (61) |
11.64 (27) |
21.66 (41) |
18.00 (54) |
| From 60 a 69 |
16.15 (130) |
13.22 (68) |
51.18 (201) |
23.28 (53) |
14.41 (27) |
14.07 (42) |
| From 70 a 79 |
24.32 (196) |
12.93 (67) |
10.75 (42) |
21.46 (49) |
13.64 (26) |
16.30 (49) |
| From 80 a 89 |
9.42 (76) |
7.39 (38) |
6.21 (24) |
9.90 (23) |
6.87 (13) |
7.00 (21) |
| From 90 a 99 |
3.09 (25) |
1.52 (8) |
1.62 (6) |
5.07 (12) |
4.45 (8) |
0.54 (2) |
| Sex |
|
|
|
|
|
|
| Femele |
37.38 (301) |
45.90 (236) |
20.01 (79) |
44.26 (102) |
45.07 (85) |
37.02 (111) |
| Male |
62.62 (504) |
54.10 (278) |
79.99 (314) |
55.74 (128) |
54.93 (103) |
62.82 (189) |
| Regime |
|
|
|
|
|
|
| Contributory |
32.72 (263) |
34.17 (176) |
34.41 (135) |
26.68 (61) |
35.59 (67) |
34.7 (104) |
| Subsidized |
66.53 (536) |
63.96 (329) |
64.01 (251) |
69.83 (160) |
61.80 (116) |
61.8 (186) |
| Bound |
0.75 (6) |
1.87 (10) |
1.57 (6) |
3.48 (8) |
2.61 (5) |
3.5 (10) |
| Social stratum |
76.20 (613) |
75.37 (388) |
75.73 (297) |
76.88 (177) |
80.56 (151) |
73.4 (221) |
| Low [1 y 2] |
76.20 (613) |
75.37 (388) |
75.73 (297) |
76.88 (177) |
80.56 (151) |
73.4 (221) |
| Medium [3 y 4] |
23.40 (188) |
24.20 (125) |
24.13 (95) |
22.64 (52) |
19.15 (36) |
26.3 (79) |
| High [5 y 6] |
0.41 (3) |
0.42 (2) |
0.14 (1) |
0.48 (1) |
0.29 (1) |
0.3 (1) |
| Origin |
|
|
|
|
|
|
| Risaralda |
86.11 (693) |
83.64 (430) |
90.37 (355) |
92.24 (212) |
85.88 (161) |
87.1 (262) |
| Other departments |
13.89 (112) |
16.36 (84) |
9.63 (38) |
7.76 (18) |
14.12 (27) |
12.9 (39) |
PFS: Functional Patterns of Health
The PFS Elimination, Perceived health management, and Activity/exercise predominate in older adults, while the Nutritional, Metabolic, and Cognitive-Perceptual PFS are more frequent in adults under 65 years of age. Analysis of trends in PFS with respect to age groups showed that PFS.4 Activity and exercise is the most prevalent, with an upward trend with age, reaching its peak in the 70-79 age group (24.32%). PFS.2 Nutrition shows a downward trend with age, with a higher prevalence in young adults (28.23% in 30-39 age groups), gradually decreasing until reaching its lowest point in 90-99 age groups (1.52%). PFS.3 Elimination varies with age, has a significant peak in the 60-69 age group (51.18%), and is lower in young adults. The PFS.1 Health Perception-Management scores peak in the 60-69 age group and decline with increasing age; similarly, the PFS.6 Cognitive Perceptual Score scores peak in the 40-49 age group (24.08%) and trend downward with advancing age.
In general, it is observed that activity/exercise and elimination problems are the most prevalent, there is a clear age-dependent relationship in several patterns, nutrition shows an inverse trend with age.
Correlation analysis showed strong negative co-occurrences between relevant PFS, namely: Activity/ Exercise and Nutrition (-0.36), Activity /Exercise and Elimination (-0.31), Activity/Exercise and Health Perception-Management (-0.23). These negative correlations suggest that when one pattern is present, other patterns are less likely to be present; if an individual seeks interventions for activity/ exercise problems, they are less likely to report simultaneous interventions for nutrition problems; interventions for elimination problems tend not to co-occur with activity/exercise problems.
NANDA Diagnostics
Table 3 presents the distribution of the most frequent NANDA diagnoses by PFS (discrimination cri- terion: 80%). While 10 diagnoses were included in the Activity/Exercise and Nutritional/Metabolic PFS, 80% of the other patterns were represented by five or six more frequent diagnoses. The profile of Nursing diagnoses reveals that during training practices the emphasis is on minimizing the real reason for the patients' complaints, seeking better health and well-being conditions.
Table 3. Nursing Diagnoses [NANDA I]* according to relevant Functional Health Patterns identified during training practices.
X
Table 3. Nursing Diagnoses [NANDA I]* according to relevant Functional Health Patterns identified during training practices.
Relevant Functional Health Patterns Records 100% (n=11,714) |
Nursing Diagnoses [NANDA I] (Discrimination= 80%) |
% (n)** |
| 4. Activity/Exercise. Records: 37.80 (4,428) |
0032. Ineffective breathing pattern
0029. Decreased cardiac output
0085. Impaired physical mobility
0030. Impaired gas exchange
0100. Delayed surgical recovery
0093. Fatigue
0298. Decreased activity tolerance
0204. Ineffective peripheral tissue perfusion
0182. Willingness to improve self-care
0033. Impaired spontaneous ventilation
Functional pattern subtotal
Rest NANDA Pattern Activity/Exercise
|
17.55 (777)
14.86 (658)
13.39 (593)
8.90 (394)
6.73 (298)
4.95 (219)
4.67 (207)
3.97 (176)
3.18 (141)
2.19 ( 97)
80.40 (3560)
19.60 ( 868)
|
| 2. Nutritional Metabolic Records: 24.16 (2,830) |
0044. Impaired tissue integrity
0047. Impaired skin integrity
0103. Impaired swallowing
0045. Impairment of the integrity of the oral mucosa
0026. Excess fluid volume
0027. Fluid volume deficit
0179. Risk of unstable blood glucose level
0266. Risk of surgical wound infection
0312. Pressure injury in adults
0248. Risk of deterioration of the integrity of the oral mucosa
Functional pattern subtotal
Rest NANDA Nutritional/Metabolic Pattern
|
20.85 (590)
20.46 (579)
9.22 (261)
7.92 (224)
5.87 (166)
4.73 (134)
4.06 (115)
2.83 ( 80)
2.61 ( 74)
2.05 ( 58)
80.60 (2281)
19.40 (549)
|
| 3. Elimination Records: 18.43 (2,159) |
0016. Impaired urinary elimination
0023. Urinary retention
0022. Risk of urge urinary incontinence
0322. Risk of urinary retention
Functional pattern subtotal
Remainder NANDA Pattern Elimination
|
42.70 (922)
21.21 (458)
14.54 (314)
6.95 (150)
85.41 (1844)
14.58 (315)
|
| 1. Perception of Health Management Records 10.78 (1,263) |
0257. Elderly frailty syndrome
0276. Ineffective self-management of health
0043. Ineffective protection
0266. Risk of infection
0293. Willingness to improve self-management of health
0292. Ineffective health maintenance behaviors
Functional pattern subtotal
Rest NANDA P. Perception Health Management
|
21.62 (273)
15.52 (196)
15.28 (193)
15.20 (192)
10.21 (129)
8.16 (103)
85.99 (1086)
14.01 (177)
|
| 6. Cognitive/Perceptual Records 8.83 (1,034) |
0132. Acute pain
0214. Discomfort
0133. Chronic pain
0131. Memory impairment
0279. Altered thought process
Functional pattern subtotal
Rest NANDA Cognitive-Perceptual Pattern
|
41.49 (429)
17.31 (179)
13.06 (135)
5.90 ( 61)
5.90 ( 61)
83.70 (865)
16.30 (169)
|
*Source: Nursing Diagnoses: Definitions and Classification 2021-2023. 12th ed. ** Note: % = percentage in columns and n = number of records per PFS
NIC Interventions
Table 4 presents the frequency of nursing interventions by intervention domain. In the complex physiological domain, medication administration is highlighted, followed by airway management; these should be the nursing professional's greatest strengths in the clinical area. In the basic physiological domain, according to the diagnostic profile, urinary elimination management and assistance with self-care are highlighted. In the behavioral domain, teaching and patient agreement predominate, and in the safety domain, infection control and skin surveillance predominate. NIC interventions during nursing training are fully articulated with the PFS and nursing diagnoses relevant to the adult and older adult population.
Table 4. Nursing Interventions (NIC) according to Domain
X
Table 4. Nursing Interventions (NIC) according to Domain
| NIC Domains Registrations 100% (n=1,714) |
Nursing Interventions (NIC) |
% (n)* |
| Complex Physiological Records: 39.29 (4,603) |
Medication administration
Airway management/Monitoring/Oxygen therapy
Cardiac Care: Rehabilitation/Acute/Arrhythmia
Wound/skin/access care/monitoring
Fluid Management - Electrolytes/Monitoring/Dialysis
Circulatory care: venous/arterial insufficiency
NIC remainder complex physiological domain
|
48.97 (254)
13.62 (627)
13.12 (604)
7.63 (351)
6.52 (300)
4.24 (195)
5.91 (272)
|
| Basic Physiological Records: 25.99 (3,045) |
Urinary elimination management/ retention care/ incontinence care
Help with self-care
Nutrition Management
Exercise promotion/ Weight loss aid
Acute/Chronic/Positional Pain Management
Exercise/activity/relaxation therapy
Maintenance/Restoration of oral health
Rest NIC basic physiological domain
|
24.86 (757)
17.50 (533)
15.96 (486)
12.15 (370)
13.50 (411)
6.67 (203)
5.91 (180)
3.09 ( 94)
|
| Behavioral Records: 19.04%(2,230) |
Teaching: individual/: medications /: disease process/ Health education
Emotional support/Mood management
Patient Agreement/Spiritual Support
Sexual counseling
Decreased anxiety
Help in self-modification
Cognitive stimulation
Rest NIC behavioral domain
|
29.19 (651)
19.82 (442)
18.52 (413)
12.56 (280)
8.16 (182)
3.32 (74)
1.97 (44)
6.46 (144)
|
| Security Records: 7.52%(881) |
Infection control/Infection protection
Risk identification
Surveillance
Isolation/Validation Therapy
Triage: emergency center
Dementia management
Rest NIC domain security
|
54.60 (481)
18.16 (160)
8.17 (72)
7.26 (64)
6.58 (58)
1.14 (10)
4.08 (36)
|
| Health System Records: 4.40% (516) |
Orientation in the health system
Interpretation of laboratory data
Sample handling
Health care information exchange
Discharge Planning
Rest NIC domain Health System
|
26.74 (138)
21.32 (110)
13.95 (72)
13.95 (72)
13.18 (68)
10.85 (56)
|
| Family Records: 3.75% (439) |
Promote family involvement
Maintaining family processes
Stimulation of family integrity
Family therapy
Family mobilization
|
51.48 (226)
20.50 (90)
20.50 (90)
7.29 (32)
5.47 (24)
|
*Nota: % = porcentaje en columnas y n= número de registros por Dominio NIC
Discussion
In line with the objective of this study, the indicators from the National Observatory on Aging and Old Age show that, in Risaralda, in 2022, the morbidity treated in people over 60 years of age was mainly due to diseases of the circulatory system and Diabetes, which were more common in women; fo- llowed by diseases of the urinary system, communicable diseases, and the respiratory system, which were more prevalent in men21. Consistent with the above, in our study, the highest proportions of interventions were concentrated in Activity /Exercise, Nutritional Metabolism, Elimination, Health Perception/Management, and Cognitive/Perceptual. This result demonstrates that the nursing training practices in the clinical area at the selected university institution do respond to the regional guidelines for health care during adulthood and old age, in terms of morbidity. The interventions are aimed at minimizing functional dependency and disability and improving the quality of life of older adults, as outlined in the Colombian Policy on Aging and Old Age8.
As observed in the frequency of PFS, Nursing Interventions (NIC) for the adult and older adult population, delivered during training practices, correspond to the professional training needs and management guidelines for the most prevalent events in this population. Thus, the largest proportions correspond to medication administration, airway management, urinary elimination management, assistance with self-care, patient education and agreements, infection control, and skin surveillance.
Training practices in health allow the integration of theoretical and practical knowledge; this contributes to a more complete humanistic and professional training22. These educational experiences, when aligned with NIC interventions, as shown in this study, favor the development of competencies for the comprehensive and integrated care of health/illness experiences, promo- ting ethical and people-centered interventions, which at any time in their lives are oriented towards healthy aging.
Similarly, recent research23,24 addresses nursing care practices in adults and older adults, highlighting the importance of interventions focused on promoting mobility and improving nutritional status to prevent functional decline. Chronic diseases such as Hypertension, Diabetes, and heart disease are commonly associated with decreased physical function in this population3. Consistently, during the training practices recorded in this study, a predominance of interventions in the "Activity and exercise" and "Nutrition-metabolic" patterns was observed.
Maintaining regular physical activity not only improves functional capacity but also contributes to the preservation of cognitive and physical reserve in older adults, resulting in greater independence and quality of life25. Finding this pattern relevant in this study means that students are acquiring skills to promote physical activity and prevent functional decline, thus contributing to comprehensive patient-centered care.
On the other hand, recent studies with biomarkers26 have indicated that socioeconomic conditions throughout life decisively affect health in old age, mainly in the increase of cardiovascular risk. The findings of this study show a population attended for chronic non-communicable diseases of cardiovascular and metabolic type, coming from strata 1 and 2 and with a subsidized insurance regime.
Conclusions
The predominance of adult and elderly patients treated under the subsidized system from low socioeconomic strata and the high percentage of interventions targeted at them reflect the influence of socioeconomic profile on access to health care. Care strategies emanating from public policies are essential to reducing inequalities and improving the well-being of these individuals.
The analysis of the nursing training practice information system at the selected institution highlights the importance of using PFS in assessing the health status of the populations served. The integration of NANDA Diagnoses and NIC Interventions allows for identifying the competencies nursing students are developing for the comprehensive care of adults and older adults, and in turn, orienting interventions toward healthy aging policies.
The most frequent NIC interventions focused on the PFS of Activity and Exercise, Nutritional- Metabolic, Elimination, Health Perception/Management, and Cognitive/Perceptual; this coincides with the morbidity profile described by the National Observatory on Aging and Old Age, which allows us to conclude that the nursing training practices in the clinical area at the selected university institution do respond to the guidelines for health care during adulthood and old age in the region.
Regarding Nursing Interventions, the following are highlighted, from highest to lowest proportion: Medication Administration, followed by airway management (Complex Physiological), urinary elimination management and assistance with self-care (Basic Physiological), patient education and agreement (Behavioral), infection control and skin surveillance (Safety). This intervention profile shows that Nursing Professionals at the selected Institution are acquiring key competencies required for comprehensive and effective care in the hospital setting, both in highly complex health phenomena and in basic care and health promotion in the adult and elderly population.
Conflict of interest: The authors declare that there are no conflicts of interest related to the conduct of this study or the publication of its results.
Funding: Fundación Universitaria del Área Andina- Colombia. The article is part of the institutional project CVINNO2022-GIER-GIEE-P-12675.
Acknowledgments: To the Pereira branch of the Fundación Universitaria del Área Andina for logistical support. To the nursing students and faculty responsible for data entry in the Nursing Training Practice Information System.
References
X
Referencias
Latrach-Ammar C, Febré N, Demandes I, Araneda J, González I. Importancia de las competencias en la formación de enfermería. Aquichan. 2011;11(3):305-15. https://doi.org/10.5294/AQUI.2011.11.3.5
X
Referencias
NANDA International, Inc. Diagnósticos enfermeros: definiciones y clasificación 2021-2023. 12.ª ed. Madrid: Elsevier; 2021.
X
Referencias
Wagner CM, Butcher HK, Clarke MF. Clasificación de intervenciones de enfermería (NIC). 8.ª ed. Madrid: Elsevier; 2023.
X
Referencias
Lueckmann SL, Hoebel J, Roick J, Markert J, Spallek J, von dem Knesebeck O, et al. Socioeconomic inequalities in primary-care and specialist physician visits: a systematic review. Int J Equity Health. 2021;20(1):58. https://doi.org/10.1186/s12939-020-01375-1
X
Referencias
Veldhuizen JD, Hafsteinsdóttir TB, Mikkers MC, et al. Evidence-based interventions and nurse-sensitive outcomes in district nursing care: a systematic review. International Journal of Nursing Studies Advances. 2021;3:100053. https://doi.org/10.1016/j.ijnsa.2021.100053
X
Referencias
Ministerio del Interior. Colombia. Software F_PAE. Reg. 13.61-245 del 30 de junio de 2017. Fundación Universitaria del Área Andina. 2017.
X
Referencias
Hrdlicka HC, Meise E, Corbett J, Meyer A, Grevelding P. Content Validity Testing of a Novel Cognitive Screen, the Gaylord Occupational Therapy Cognitive (GOT–Cog), to Improve Inpatient Occupational Therapy Treatment Planning. The American Journal of Occupational Therapy. 2024;78(1):7801345020. https://doi.org/10.5014/ajot.2024.050306
X
Referencias
Barón Castro MM, Muñoz Astudillo MN. Recopilación de datos NANDA, NOC, NIC 2021-2023 del Software F_PAE. V1 ed. Papyrus; 2024. https://doi.org/10.57924/LYVGIF
X
Referencias
Chois Lenis PM, Valdéz Fernández AL, Mosquera Ruiz MG, Jácome Velasco SJ, Bastidas Sánchez BE. Aprendizajes construidos por los estudiantes durante sus prácticas formativas en salud: El reconocimiento de una formación humana. Revista de Investigación Educativa. 2023;41(2):573-91. https://doi.org/10.6018/rie.548081
X
Referencias
Valenzuela PL, Morales JS, Castillo-García A, Mayordomo-Cava J, García-Hermoso A, Izquierdo M, et al. Effects of exercise interventions on the functional status of acutely hospitalized older adults: a systematic review and meta-analysis. Ageing Research Reviews. 2020;61:101-128. https://doi.org/10.1016/j.arr.2020.101076
X
Referencias
Sánchez MW, López BB. Influencia del sentido de la vida y las reservas física/cognitiva en el envejecimiento saludable/Influence of the meaning of life and the physical/cognitive reserves in healthy aging. Cauriensia Rev Anual Cienc Eclesiásticas. 2018;13:57-72. https://doi.org/10.17398/2340-4256.13.107
X
Referencias
Schmitz LL, Opsasnick LA, Ratliff SM, Faul JD, Zhao W, Hughes TM, et al. Epigenetic biomarkers of socioeconomic status are associated with age-related chronic diseases and mortality in older adults. PNAS nexus. 2025;4(4):pgaf121. https://doi.org/10.1093/pnasnexus/pgaf121
-
Pan American Health Organization. Healthy Aging [Internet] 2024 [cited 2024 Aug 2] Available from: https://www.paho.org/en/healthy-aging
-
World Health Organization. Aging and health, [Internet] 2024 [cited 2024 Aug 16] Available from: https://www.who.int/es/news-room/fact-sheets/detail/ageing-and-health
-
World Health Organization. Decade of Healthy Aging, [Internet] 2024 [cited 2024 Aug 12] Available from: https://www.who.int/es/initiatives/decade-of-healthy-ageing
-
Observatorio Nacional de Envejecimiento y Vejez - ONEV. SISPRO. Tablero de control de demografía con los indicadores de vejez y envejecimiento. Colombia. 2022. Consulta: septiembre 15, 2024. Disponible en: https://www.sispro.gov.co/observatorios/onenvejecimientovejez/ Paginas/Observatorio-Nacional-de-Envejecimiento-y-Vejez.aspx
-
Organización Panamericana de la Salud. Las cuatro áreas de acción de la Década. 2024. Consulta: septiembre 23, 2024. Disponible en: https://www.paho.org/es/decada-envejecimiento-saludable-americas-2021-2030/cuatro-areas-accion-decada
-
Ministerio de Salud y Protección Social. Plan Decenal de Salud Pública 2022-2031. Colombia. Consulta: septiembre 23, 2024. Disponible en: https://www.minsalud.gov.co/plandecenal/Paginas/PDSP-2022-2031.aspx
-
Ministerio de Salud y Protección Social. Decreto 681 de 2022. República de Colombia: 2 de mayo de 2022. Consulta: septiembre 30, 2024. p.1-51 Disponible en: https://www.minsalud.gov.co/Normatividad_Nuevo/Decreto%20No.%20681%20de%202022.pdf
-
Revista Jurídica. Se adoptó la Política de Envejecimiento y Vejez. [Internet]. 2022. Consulta: agosto 26, 2024. Disponible en: https://www.dnp.gov.co/publicaciones/Revista-Juridica/Paginas/Se-adopt%C3%B3-la-Pol%C3%ADtica-de-Envejecimiento-y-Vejez.aspx
-
Ministerio de Salud y Protección Social. Resolución 3280 de 2018. [Internet]. Colombia, 2018. Consulta: septiembre 30, 2024. Disponible en: https://www.minsalud.gov.co/Normatividad_Nuevo/Resolución%20No.%203280%20de%2020183280.pdf
-
Mostacero Morcillo E, Martínez Martín ML. Rol de la enfermera en el envejecimiento activo y saludable. Revisión narrativa. Gerokomos 2019;30(4):181-189. http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S1134-928X2019000400181&lng=es&tlng=es
-
Werezak L. What is the Nursing Process? ADPIE. Nurse.org. [Internet] 2023 [cited 2024 Sept 26]. Available from: https://nurse.org/education/nursing-process
-
Latrach-Ammar C, Febré N, Demandes I, Araneda J, González I. Importancia de las competencias en la formación de enfermería. Aquichan. 2011;11(3):305-15. https://doi.org/10.5294/AQUI.2011.11.3.5
-
NANDA International, Inc. Diagnósticos enfermeros: definiciones y clasificación 2021-2023. 12.ª ed. Madrid: Elsevier; 2021.
-
Wagner CM, Butcher HK, Clarke MF. Clasificación de intervenciones de enfermería (NIC). 8.ª ed. Madrid: Elsevier; 2023.
-
Lueckmann SL, Hoebel J, Roick J, Markert J, Spallek J, von dem Knesebeck O, et al. Socioeconomic inequalities in primary-care and specialist physician visits: a systematic review. Int J Equity Health. 2021;20(1):58. https://doi.org/10.1186/s12939-020-01375-1
-
Veldhuizen JD, Hafsteinsdóttir TB, Mikkers MC, et al. Evidence-based interventions and nurse-sensitive outcomes in district nursing care: a systematic review. International Journal of Nursing Studies Advances. 2021;3:100053. https://doi.org/10.1016/j.ijnsa.2021.100053
-
Fundación Universitaria del Área Andina. Programa de Enfermería. 2024. Consulta: septiembre 13, 2024]. Disponible en: https://www.areandina.edu.co/profesional/pereira/enfermeria
-
Ministerio del Interior. Colombia. Software F_PAE. Reg. 13.61-245 del 30 de junio de 2017. Fundación Universitaria del Área Andina. 2017.
-
Hrdlicka HC, Meise E, Corbett J, Meyer A, Grevelding P. Content Validity Testing of a Novel Cognitive Screen, the Gaylord Occupational Therapy Cognitive (GOT–Cog), to Improve Inpatient Occupational Therapy Treatment Planning. The American Journal of Occupational Therapy. 2024;78(1):7801345020. https://doi.org/10.5014/ajot.2024.050306
-
Barón Castro MM, Muñoz Astudillo MN. Recopilación de datos NANDA, NOC, NIC 2021-2023 del Software F_PAE. V1 ed. Papyrus; 2024. https://doi.org/10.57924/LYVGIF
-
Observatorio Nacional de Envejecimiento y Vejez - ONEV. SISPRO. Tablero de control para indicadores ONEV de morbilidad atendida. Colombia: 2022. Consulta: Octubre 13, 2024. Disponible en: https://www.arcgis.com/apps/dashboards/dab146035111407d8a2e06c146b017b0
-
Chois Lenis PM, Valdéz Fernández AL, Mosquera Ruiz MG, Jácome Velasco SJ, Bastidas Sánchez BE. Aprendizajes construidos por los estudiantes durante sus prácticas formativas en salud: El reconocimiento de una formación humana. Revista de Investigación Educativa. 2023;41(2):573-91. https://doi.org/10.6018/rie.548081
-
Angulo J, El Assar M, Álvarez-Bustos A, Rodríguez-Mañas L. Physical activity and exercise: Strategies to manage frailtyRedox Biol. . 2020;35:101513. https://doi.org/10.1016/j.redox.2020.101513
-
Valenzuela PL, Morales JS, Castillo-García A, Mayordomo-Cava J, García-Hermoso A, Izquierdo M, et al. Effects of exercise interventions on the functional status of acutely hospitalized older adults: a systematic review and meta-analysis. Ageing Research Reviews. 2020;61:101-128. https://doi.org/10.1016/j.arr.2020.101076
-
Sánchez MW, López BB. Influencia del sentido de la vida y las reservas física/cognitiva en el envejecimiento saludable/Influence of the meaning of life and the physical/cognitive reserves in healthy aging. Cauriensia Rev Anual Cienc Eclesiásticas. 2018;13:57-72. https://doi.org/10.17398/2340-4256.13.107
-
Schmitz LL, Opsasnick LA, Ratliff SM, Faul JD, Zhao W, Hughes TM, et al. Epigenetic biomarkers of socioeconomic status are associated with age-related chronic diseases and mortality in older adults. PNAS nexus. 2025;4(4):pgaf121. https://doi.org/10.1093/pnasnexus/pgaf121