Rev Cuid. 2025; 16(3): e4768
Abstract
Introduction: Studies attempting to predict empathy based on resilience are characterized by incomplete theories of both constructs and focus on obtaining empirical evidence.
Objective: To verify whether resilience can predict empathy.
Materials and Methods: A cross-sectional construct validity study was conducted. Salvadorean nursing students were assessed using the Jefferson Scale of Empathy-Health Professions Students (JSE-HPS) and the Engineering, Ecological and Adaptive (EEA) resilience scale. Psychometric analyses (confirmatory factor analysis, reliability, and invariance) were conducted, and prediction was assessed using structural equations.
Results: The compliance of the model of both constructs and the reliability of the data were verified. Some dimensions of resilience positively predicted the dimensions of empathy, while others predicted them negatively.
Discussion: Ecological resilience and engineering resilience positively predicted all the dimensions of empathy. However, adaptive resilience negatively predicted empathy, suggesting that students may lack sufficiently developed adaptive traits to prevent declines in "compassionate care" and "standing in the patient's shoes." Therefore, their ability to connect emotionally and understand the patient's situation is hampered by a deficit of the traits that support adaptation to new situations.
Conclusion: Empathy and resilience education cannot be independent of each other. On the contrary, resilience exerts a protective effect that enables the free expression of empathy that students have developed over the course of their lives.
Keywords:
Resilience, Psychological; Empathy; Psychometrics; Reproducibility of Results; Students; Vocational Education
Resumen
Introducción: Los estudios que intentan predecir la empatía a partir de la resiliencia se caracterizan por teorías incompletas de ambos constructos y por centrarse principalmente en la obtención de evidencia empírica.
Objetivo: Comprobar si la resiliencia puede predecir la empatía.
Materiales y Métodos: Estudio de corte transversal y de validez de constructo. Se evaluó a estudiantes salvadoreños de Enfermería mediante la Jefferson Scale of Empathy–Health Professions Students (JSE-HPS) y la Engineering, Ecological and Adaptive (EEA). Se llevaron a cabo análisis psicométricos (análisis factorial confirmatorio, confiabilidad e invarianza) y la predicción se evaluó mediante ecuaciones estructurales.
Resultados: Se verificó el cumplimiento del modelo en ambos constructos y la confiabilidad de los datos. Algunas dimensiones de resiliencia predijeron positivamente las dimensiones de la empatía, mientras que otras lo hicieron de manera negativa.
Discusión: La resiliencia ecológica y la de ingeniería predijeron positivamente todas las dimensiones de la empatía. Sin embargo, la resiliencia adaptativa predijo negativamente la empatía, lo que sugiere que los estudiantes no tienen los rasgos adaptativos suficientemente desarrollados para evitar disminuciones en “cuidado compasivo” y “ponerse en el lugar del paciente”. En consecuencia, su capacidad para conectarse emocionalmente y comprender la situación del paciente se ve limitada por un déficit en los rasgos que favorecen la adaptación a nuevas situaciones.
Conclusión: La formación en empatía y resiliencia no puede abordarse de manera independiente. Por el contrario, la resiliencia ejerce un efecto protector que permite la libre expresión de la empatía desarrollada por los estudiantes a lo largo de su vida.
Palabras Clave:
Resiliencia Psicológica; Empatía; Psicometría; Reproductibilidad de Resultados; Estudiantes; Formación Vocacional
Resumo
Introdução: Estudos que buscam predizer a empatia com base na resiliência são caracterizados por teorias incompletas de ambos os construtos e se concentram na obtenção de evidências empíricas.
Objetivo: Testar se a resiliência pode predizer a empatia.
Materiais e Métodos: Foi realizado um estudo transversal de validade de construto. Estudantes de enfermagem colombianos foram avaliados por meio da Escala Jefferson de Empatia para Estudantes de Ciências da Saúde e da Escala de Resiliência Individual. Utilizou-se análise psicométrica (análise fatorial confirmatória, confiabilidade e invariância), e a predição foi realizada por meio de equações estruturais.
Resultados: A conformidade do modelo de ambos os construtos e a confiabilidade dos dados foram verificadas. Constatou-se que algumas dimensões previram positivamente as dimensões da empatia, enquanto outras as previram negativamente.
Discussão: A resiliência ecológica e a resiliência da engenharia, especificamente, predizem positivamente todas as dimensões da empatia. No entanto, a resiliência adaptativa a prediz negativamente. Esta última situação implica que os estudantes não possuem traços adaptativos suficientemente desenvolvidos para evitar um declínio nas dimensões do cuidado compassivo e de "colocar-se no lugar do paciente". Portanto, sua capacidade de se conectar emocionalmente e compreender a situação do paciente é prejudicada por um déficit nas características que permitem a adaptação à nova situação.
Conclusão: O treinamento em empatia e resiliência não podem ser independentes. Pelo contrário, o efeito protetor da resiliência permite a livre expressão da empatia que o aluno desenvolveu ao longo da vida.
Palavras-Chave:
Resiliência Psicológica; Empatia; Psicometria; Reprodutibilidade dos Testes; Estudantes; Educação Vocacional
Introduction
Empathy is an attribute that enables interaction between Nursing professionals and patients
(intersubjectivity)1. Through this interrelationship, Nursing professionals are able to understand
the subjectivity of patients' thoughts, comprehend intellectually or imaginatively their conditions,
and experience patients' emotions as if they were their own, but without renouncing the principle
of objectivity and avoiding emotional contagion2. The described situation gives patients the
opportunity to feel that their health condition is understood, helping to establish deeper bonds
with the Nursing professional3. This situation benefits patients, Nursing professionals, and the
comprehensive therapeutic process. All these benefits have been extensively described in several
studies4,5. Consequently, empathy is an important contributing factor, along with other factors, in
establishing a solid foundation for the development and implementation of humane patient care6.
The emergence and development of empathy can only be explained from both an evolutionary
perspective (phylogeny) and an individual's life experience (ontogeny)7. Empathy is an attribute
characterized by genetic inheritance rooted in phylogenetic processes and by the extent to which
this inheritance is expressed through ontogenetic processes8. While phylogeny provides the genetic
possibility of developing empathy (genetic makeup), ontogeny determines if that possibility can reach
various stages of development. This suggests that ontogenetic processes are directly related to the
development of empathic capacity in an individual. The empathy ultimately "achieved" depends on
numerous factors influencing development9, beginning in early childhood and continuing until the
neural structures that enable the development of positive emotions (limbic system)10 and cognitive
abilities (prefrontal and temporal cortex) are fully developed in young adulthood11. Both facets of
empathy evolve in parallel. Therefore, empathy development is a process that begins naturally in
early childhood and continues until the neural architecture of young adults is consolidated12. As a
result, one of the last (and most important) windows of opportunity for cultivating empathy aligned
with the professional role of nurses is during their university education.
There are two fundamental stages for ensuring that empathy education for Nursing students has a
greater chance of success. The first stage involves conducting an empathy "diagnosis." This diagnosis
involves evaluating empathy levels, including cognitive and emotional components, and identifying
strengths and weaknesses during the diagnosis. It is followed by a parallel analysis that examines
factors that could theoretically have a positive or negative impact on empathy, such as resilience. Such
a diagnosis could lead us to recognize that an effective diagnosis of empathy not only depends on
the empathy that students have developed throughout their lives before entering university, but also
includes assessing how certain factors may contribute to explaining it. Consequently, a serious and
responsible intervention would not only include all the necessary elements in the teaching-learning
process to consolidate empathy education, but also the need to introduce the factors shown to be
predictors of empathy into the aforementioned processes. In line with this rationale, the present study
aimed to determine whether the dimensions of resilience can predict the dimensions of empathy in
Nursing students.
Materials and Methods
Design
This was a non-experimental, cross-sectional, psychometric study with construct validity.
Population
The study population comprised Nursing students enrolled in the Faculty of Health Sciences at the
Universidad Evangélica de El Salvador (El Salvador) (n=160).
Sample
The sample consisted of 110 students assessed in May 2024, representing 68.75% of the total
population. Although this sample was not randomly selected, it included almost the entire population;
therefore, the results can be extrapolated to the population under study.
Variables
Resilience was considered the independent variable, and empathy the dependent variable.
Eligibility criteria
Inclusion. Students who voluntarily expressed their desire to participate in this research and signed
the informed consent form were included.
Exclusion. Students who did not attend classes on the day of data collection or those who completed
the instruments but did not sign the informed consent form were excluded from the study.
Instruments
Individual resilience
Trait resilience scale. The Engineering, Ecological, and Adaptive (EEA) resilience scale13 assesses
three facets of resilience: engineering (items 1–4), ecological (items 5–8), and adaptive (items 9–12).
This scale consists of 12 items rated on a 5-point Likert scale ranging from "Strongly disagree" (1) to
"Strongly agree" (5). The EEA resilience scale has demonstrated satisfactory internal consistency and
test-retest reliability (MacDonald's omega = 0.70–0.86; Cronbach's alpha = 0.68–0.82). Furthermore,
this scale exhibits a stable cross-cultural factor structure, convergent and construct validity in relation
to personality traits, and a positive contribution to clinical and non-clinical psychological health
statuses13.
Empathy
Jefferson Scale of Empathy-Health Professions students (JSE-HSS)14,15. This scale comprises 20 items
that measure empathy levels in health science students across various specialties. Items are rated
on a 7-point Likert scale ranging from 1 (strongly disagree) to 7 (strongly agree). The scale measures
three dimensions: compassionate care (CC; items 1, 7, 8, 11, 12, 14, 18, 19); perspective taking (PT;
items 2, 4, 5, 9, 10, 13, 15, 16, 17, 20); and standing in the patient's shoes (SPS; items 3 and 6). PT and
SPS dimensions constitute the cognitive component of empathy, whereas CC reflects the emotional
component of this construct. The scale has demonstrated adequate internal consistency (α = 0.78–
0.92) and appropriate correlations with other psychological variables15.
Both instruments underwent cultural adaptation through the following processes: translation and
back-translation (translation from the original English to Spanish and from Spanish into English),
expert panel review of the translation, and finally, pilot testing with 20 volunteer students from the
study population to verify content comprehension.
Procedure
Students were assessed in classrooms, in a formal academic setting, using an online questionnaire.
The instruments were administered by properly trained educators who ensured students' voluntary
participation.
Statistical analysis
Descriptive statistics (mean, standard deviation, skewness, and kurtosis) were calculated for both
variables and their dimensions. For continuous quantitative variables, normality was tested using the
Kolmogorov-Smirnov test (K-S; n>50).
Confirmatory Factor Analysis (CFA) was performed using the robust maximum likelihood estimator in
a multiple linear regression (MLR) analysis16,17, as the items had more than five response categories18.
Model fit was evaluated using the following criteria: root mean square error of approximation (RMSEA
< 0.08), standardized root mean squared error (SRMR < 0.08), comparative fit index (CFI > 0.95), and
Tucker-Lewis Index (TLI > 0.95)19,20. Internal consistency of the scale was assessed using Cronbach's
alpha21 and McDonald's omega coefficients22, with values > 0.70 considered acceptable23.
All analyses described were conducted in R (RStudio interface) using the following packages: lavaan
version 0.6-17, psych version 2.4.1, semTools version 0.5-6, and MVN version 5.9. Statistical
significance was set at p < 0.05 (α = 0.05). All data collected are freely available for access and
consultation at OSFHOME24.
Ethical considerations
This study was approved by the Research Directorate and the Health Research Ethics Committee of
the Universidad Evangélica de El Salvador (CEIS-UEES), Minutes No. 018 of April 2024. Participating
students considered minors (age < 18 years) completed the instrument only after prior parental
consent was obtained. The study was classified as minimal risk.
Resultados
The age data were normal (p >0.05). The sample represented 68.75% of the total population. The
distribution by sex was 20.00% male (n = 22) and 80.00% female (n = 88). The mean age of male
students was 23.59 years (SD = 3.92), whereas the mean age of female students was 22.89 years (SD =
4.72). Table 1 presents mean, standard deviation, skewness, and kurtosis estimates for each construct
studied and its respective dimensions. The skewness and kurtosis estimates are within acceptable
ranges.
Table 1. Descriptive results of the studied constructs and their corresponding dimensions.
n=110
X
Table 1. Descriptive results of the studied constructs and their corresponding dimensions.
n=110
|
Minimum |
Maximum |
M ± SD |
Skewness |
Standard
error |
Kurtosis |
Standard
error |
| Empathy |
70 |
127 |
97.38 ± 13.851 |
0.200 |
0.230 |
-0.954 |
0.457 |
| Compassionate care |
8 |
53 |
31.66 ± 10.986 |
-0.591 |
0.230 |
-0.197 |
0.457 |
| Perspective taking |
27 |
70 |
59.25 ± 9.421 |
-1.184 |
0.230 |
1.440 |
0.457 |
| Standing in the patient's shoes |
2 |
14 |
6.46 ± 2.515 |
0.179 |
0.230 |
-0.113 |
0.457 |
| Resilience |
28 |
60 |
44.44 ± 8.208 |
0.158 |
0.230 |
-0.833 |
0.457 |
| Engineering resilience |
4 |
20 |
13.56 ± 3.974 |
-0.233 |
0.230 |
-0.758 |
0.457 |
| Ecological resilience |
4 |
20 |
16.15 ± 3.118 |
-1.037 |
0.230 |
1.588 |
0.457 |
| Adaptative resilience |
4 |
20 |
14.73 ± 3.332 |
-0.442 |
0.230 |
0.426 |
0.457 |
M = Mean; SD = Standard Deviation
Measurement models
The present study found that the scale of empathy presents adequate model fit indices (χ2 = 261.00; df
= 165; p < 0.001; RMSEA = 0.075, 90% CI [0.056 – 0.093]; CFI = 0.90; TLI = 0.88; SRMR = 0.099),
supporting validity based on internal structure. Regarding reliability, all dimensions of the scale show
acceptable internal consistency: perspective taking (ω = 0.90; α = 0.89), compassionate care
(ω = 0.87; α = 0.84), and standing in the patient's shoes (ω = 0.52; α = 0.51).
In relation to the resilience scale, this instrument also showed strong evidence of validity based on
internal structure (χ2 = 79.55; df = 51; p = 0.006; RMSEA = 0.076, 90% CI [0.037 – 0.110]; CFI = 0.95;
TLI = 0.93; SRMR = 0.063). In addition, it showed adequate and acceptable reliability across all
dimensions: Engineering (ω = 0.88; α = 0.87), ecological (ω = 0.84; α = 0.84), and adaptive
(ω = 0.79; α = 0.79). All these results show that both measurement models (empathy and resilience)
are adequately represented and are suitable for the structural model.
Explanatory model
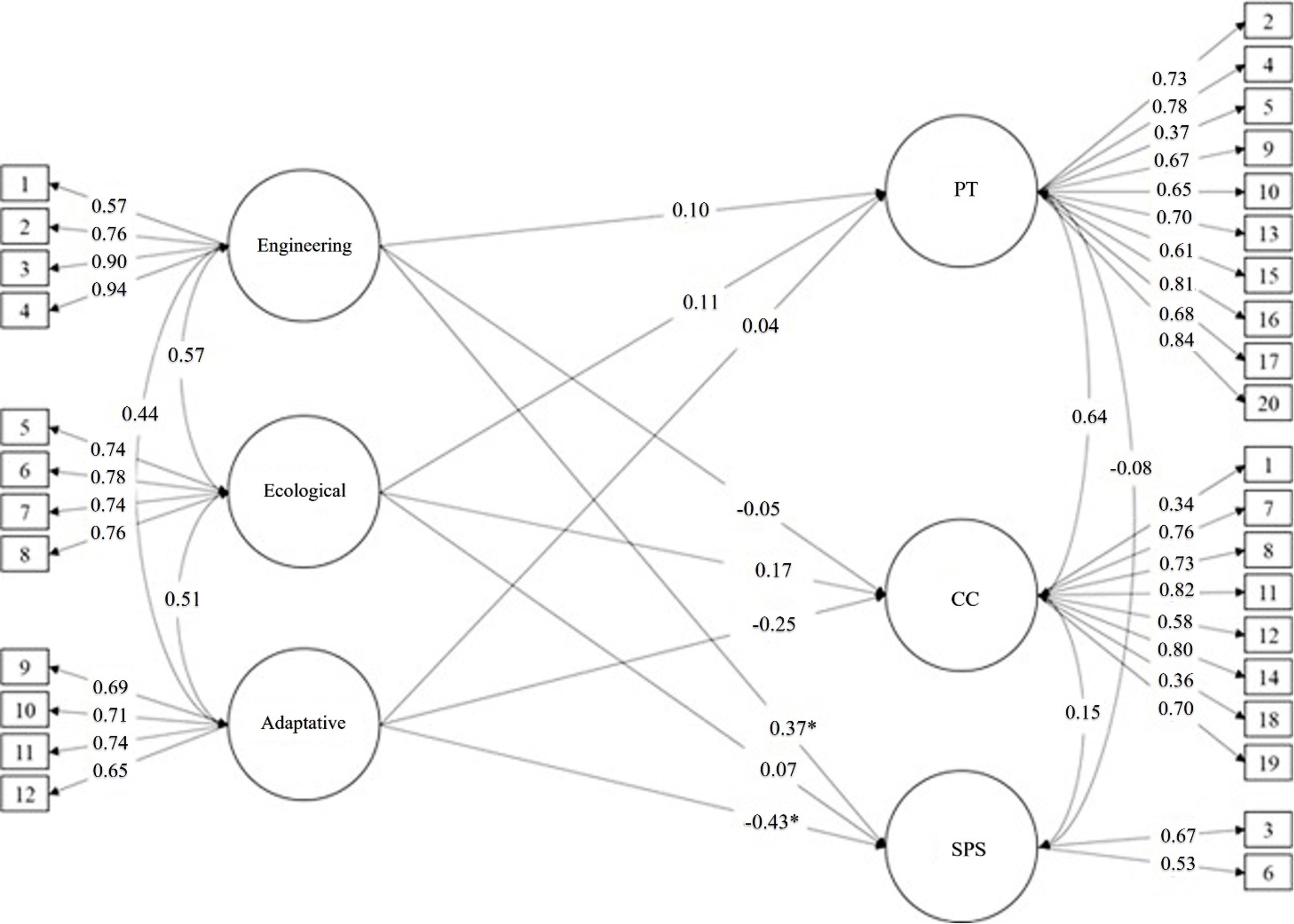
The present study showed that the structural model presents acceptable fit indices (χ2 = 658.46; df
= 447; p < 0.001; RMSEA = 0.065, 90% CI [0.053 – 0.076]; CFI = 0.88; TLI = 0.86; SRMR = 0.086). As
shown in Figure 1, the engineering resilience dimension did not significantly predict empathy
dimensions, except for the "standing in the patient's shoes" dimension (0.37). Regarding the ecological
dimension, Figure 1 shows that it did not significantly predict the dimensions of empathy.
Furthermore, the adaptive dimension significantly predicted only standing in the patient's shoes
dimension (0.43).
Discusion
The results of the psychometric study confirmed that the data collected for both constructs
demonstrated internal validity and reliability. Therefore, the analyses derived from these conditions
will not be characterized by biases attributable to internal structure validity25. This process should be
considered a standard methodological routine in all studies that employ measurement instruments
to assess attributes, such as those analyzed in this study.
The concept of resilience generally expresses the personal and interpersonal capacities and internal
strengths that enable learning and growth in the face of adverse circumstances. Some authors
conceptualize resilience as a dynamic construct encompassing a broad range of phenomena that
enable successful adaptation to threats that might otherwise hinder personal development26. Although
resilience requires an individual response, it is not exclusively an individual characteristic since it is
shaped by the interplay of individual and environmental factors. When these factors converge, they
may themselves become sources of threat. In the context of Nursing education, students consistently
encounter highly demanding situations that compel them to confront themselves. Such confrontation
creates the conditions for students to recognize their potential and abilities, thereby strengthening
themselves, learning, and responding effectively to disruptive circumstances encountered during
professional practice27.
Within this general framework, the results reported in this article should be analyzed, and the analysis
should include how resilience characteristics among Nursing students may predict empathy. In this
regard, it should be emphasized that the three dimensions assessed by the resilience instrument
represent three different but continuous moments. Partial success in one of them will not guarantee
an adequate resilient response; rather, a positive resilient response depends on consistent success
across all three moments. However, it should be noted that a positive resilient response does not
necessarily translate into higher empathy, as the process of developing empathy follows its own path
and distinct characteristics. The function of resilience is to cope with disruptions in such a way that
the empathy attained by the student, whether high or low, is not affected.
Ecological resilience reflects the ability to resist and absorb a disturbance before reorganizing essential
defense mechanisms to maintain equilibrium at critical levels. It is, therefore, the first response to a
disturbance. The results of this study showed that ecological resilience positively predicted all three
dimensions of empathy, suggesting that students may possess traits associated with the ability to
endure negative events. Such traits include robustness, confidence in one's strengths and abilities,
stoicism, resourcefulness, and determination in coping with negative events throughout life28,29.
These traits must be sufficiently strong so as not to affect any of the dimensions of empathy. This
means that these traits associated with this dimension appear to have the property of not affecting
the ability to engage emotionally and act to help the patient (CC); the ability to understand the
patient's condition intellectually or imaginatively (PT); and the ability to appreciate the subjectivity
of the patient's thoughts (SPS). It should be noted that the mean score observed for this dimension
of resilience was 16.15 (Table 1), which indicates that there is room for considering the need to
strengthen this dimension.
Engineering resilience refers to an individual's ability to recover or "bounce back" to baseline following
adverse experiences30,31. Consequently, it is the ability to return to the initial state after suffering a
negative event. It thus represents the "second moment" of resilient response. This dimension has
been positively associated with "spirituality" and "emotional intelligence," some of the specific traits
of this dimension31. In the present study, engineering resilience positively predicted AT and SPS (i.e.,
the cognitive component) but negatively predicted CC. However, the negative predictive value was
low (Figure 1), suggesting that its effect is small. The observed mean score for this dimension was
13.56, which shows that there are still opportunities for further development in this dimension.
Adaptive resilience reflects the ability to adapt effectively to changes caused by disruption, adjust
to circumstances, be flexible, change according to events, solve problems innovatively, constantly
attempt to positively transform adverse aspects, and respond to disruptions with strength and
moderation32,33. Adaptive resilience represents the "third moment" of resilient response. The results
observed in relation to this dimension showed that adaptive resilience primarily predicted CC and
SPS negatively. The relatively low mean score in this dimension (14.73; Table 1) may reduce students'
emotional engagement at a given moment and, therefore, reduce their ability to assist patients.
Moreover, it may diminish their ability to understand the subjectivity of patients' thoughts, thereby
limiting their ability to feel and understand the patient's condition, hindering natural patient-student
interactions, and, in the future, affecting the professional's natural activity with the patient.
Overall, the results observed in this study point to deficits in resilience education, particularly in
adaptive resilience. These results are relevant to the professional future of Nursing students because
they limit their chances of successfully coping with disturbances encountered during their Nursing
practice34-36. In parallel, the empathy scores observed, when compared with established cut-off points
for Latin American students37, suggest potential for further growth. Specifically, overall empathy
scores and their dimensions were as follows: Empathy = 97.38 (high); CC = 31.66 (medium); AT =
59.25 (high), and SPS = 6.46 (medium). These results may hinder the educational initiatives aimed at
cultivating the capacities required for humane patient care37,39.
Although not the primary objective of this study, it is necessary to point out that resilience, like
empathy, can be enhanced through educational actions40-43. Therefore, these results should be
considered by the institution responsible for the education of the participating students to improve
their curriculum. Regardless of the specific findings of this study, the predictive role of resilience for
empathy appears to be a general phenomenon44. Despite the scarcity of research of this type in Latin
America, fostering education about resilience and empathy in Nursing students should be regarded
as part of the social responsibility of higher education institutions45-47. Additionally, coping strategies
for adverse events should also be taught.
Strengths and limitations
This study is characterized by an evaluation of the measurement model as a prerequisite for ensuring
that the values of empathy and resilience (and their respective dimensions) are not biased by errors
arising from non-compliance with the measurement model. As a result, the predictive values for some
dimensions are robust compared to others. However, the sample cannot be considered representative
of the target population, as the study characteristics did not allow for mandatory participation of
students in completing the administered instruments.
Conclusion
The findings indicate that the dimensions of resilience predict the dimensions of empathy. Nursing
education institutions should therefore integrate resilience and empathy education into their
curricula.
Conflict of interest: The authors declare no conflict of interest.
Funding: This research received no funding.
References
XReferencias
Castellón-Montenegro H, Barraza-Ospino D, Borré-Ortiz YM, Lastre-Amell G, Erazo-Coronado AM, Díaz-Narváez VP. Empathy in nursing students from the Metropolitana University of Barranquilla (Colombia). Texto Contexto Enferm. 2020;29:e20180314. https://doi.org/10.1590/1980-265X-TCE-2018-0314
XReferencias
Ebisch SJH, Scalabrini A, Northoff G, Mucci C, Sergi MR, Saggino A, et al. Intrinsic Shapes of Empathy: Functional Brain Network Topology Encodes Intersubjective Experience and Awareness Traits. Brain Sci. 2022;12(4):477. https://doi.org/10.3390/brainsci12040477
XReferencias
Troncoso A, Blanco K, Rivera-Rei Á, Martínez-Pernía D. Empathy bodyssence: temporal dynamics of sensorimotor and physiological responses and the subjective experience in synchrony with the other's suffering. Front Psychol. 2024;15:1362064. https://doi.org/10.3389/fpsyg.2024.1362064
XReferencias
Chengappa N, Rajkumar Honest PC, David K, Pricilla RA, Rahman SM, Rebecca G. Effect of BATHE interview technique on patient satisfaction in an ambulatory family medicine centre in South India. Fam Med Community Health. 2020;8(4):e000327. https://doi.org/10.1136/fmch-2020-000327
XReferencias
Gonzalez-Liencres C, Shamay-Tsoory SG, Brüne M. Towards a neuroscience of empathy: ontogeny, phylogeny, brain mechanisms, context and psychopathology. Neurosci Biobehav Rev. 2013;37(8):1537-48. https://doi.org/10.1016/j.neubiorev.2013.05.001
XReferencias
Díaz-Narváez VP, Calzadilla-Núñez A, Alonso LM, Torres-Martínez PA, Cervantes-Mendoza M, Fajardo-Ramos E. Empathy and ontogeny: a conceptual approach. West Indian Med J. 2017;66(3):1-4. https://www.mona.uwi.edu/fms/wimj/article/3107
XReferencias
Tang Y, Wang C, Li Q, Liu G, Song D, Quan Z, et al. Neural Network Excitation/Inhibition: A Key to Empathy and Empathy Impairment. Neuroscientist. 2024;30(6):644-65. https://doi.org/10.1177/10738584231223119
XReferencias
Veerareddy A, Fang H, Safari N, Xu P, Krueger F. Cognitive empathy mediates the relationship between gray matter volume size of dorsomedial prefrontal cortex and social network size: A voxel-based morphometry study. Cortex. 2023;169:279-89. https://doi.org/10.1016/j.cortex.2023.09.015
XReferencias
Maltby J, Day L, Hall S. Refining Trait Resilience: Identifying Engineering, Ecological, and Adaptive Facets from Extant Measures of Resilience. PLoS One. 2015;10(7):e0131826. https://doi.org/10.1371/journal.pone.0131826
XReferencias
Hojat M, DeSantis J, Shannon SC, Mortensen LH, Speicher MR, Bragan L, et al. The Jefferson Scale of Empathy: a nationwide study of measurement properties, underlying components, latent variable structure, and national norms in medical students. Adv Health Sci Educ Theory Pract. 2018;23:899-920. https://doi.org/10.1007/s10459-018-9839-9
XReferencias
Tzialla N, Boka V, Menexes G, Kotsanos N, Arapostathis K. Psychometric properties of the Greek version of the Jefferson Scale of Empathy and empathy levels in Greek dental postgraduate students. Eur Arch Paediatr Dent. 2023;24(6):691-70. https://link.springer.com/article/10.1007/s40368-023-00826-x
XReferencias
Yuan KH, Bentler PM. Three likelihoodbased methods for mean and Covariance structure analysis with nonnormal missing data. Sociol Methodol. 2000;30(1):165–200. https://doi.org/10.1111/0081-1750.00078
XReferencias
Rhemtulla M, Brosseau-Liard PE, Savalei V. When can categorical variables be treated as continuous? A comparison of robust continuous and categorical SEM estimation methods under suboptimal conditions. Psychol Methods. 2012;17(3):354–33. https://doi.org/10.1037/a0029315
XReferencias
Kline RB. Principles and Practice of Structural Equation Modeling (4th ed.). 2016. The Guilford Press.
XReferencias
Schumacker RE, Lomax RG. A Beginner’s Guide to Structural Equation Modeling: Fourth Edition (4th ed.). 2015. Routledge.
XReferencias
McDonald RP. Test Theory: A Unified Treatment. 1999. Taylor & Francis.
XReferencias
Díaz-Narváez VP, Vallecampo Contreras A, Campos de Chavarría, Estrada-Méndez N, Sánchez de Elías DA, Vilca LW, Reyes-Reyes A, Gamarra-Moncayo J. La resiliencia, predictor de la empatía en estudiantes de Enfermería. OSFHOME. 2025. https://doi.org/10.17605/OSF.IO/AE5XH
XReferencias
Mylonas K, Furnham A. Bias in terms of culture and a method for reducing it: An eight-country “Explanations of Unemployment Scale” study. Educ Psychol Meas. 2014;74(1):77-96. http://dx.doi.org/10.1177/0013164413502669
XReferencias
Smith BW, Dalen J, Wiggins K, Tooley E, Christopher P, Bernard J. The Brief Resilience Scale: Assessing the ability to bounce back. Int J Behav Med. 2008;15(3):194–200. https://doi.org/10.1080/10705500802222972
XReferencias
Howell KH, Miller-Graff LE. Protective factors associated with resilient functioning in young adulthood after childhood exposure to violence. Child Abuse Neglect. 2014;38(12):1985–94. https://doi.org/10.1016/j.chiabu.2014.10.010
XReferencias
Shiraishi Y, Saito Y, Kuroki T, Yoshinaga N, Tanoue H, Hayashi Y. Research and Future Challenges for Disseminating Strengths-Based Nursing and Healthcare in Japan. Nurs Leadersh. 2024;36(4):52-56. https://doi.org/10.12927/cjnl.2024.27308
XReferencias
Díaz-Narváez VP, Calzadilla-Núñez A, Reyes-Reyes A, Lastre Amell G, Castellón-Montenegro H, Andrade Valles I, et al. Empathy, psychometrics, cut-off points in nursing students from Latin America. Int Nurs Rev. 2022;70(2):185-193. https://doi.org/10.1111/inr.12783
XReferencias
Meneses-La-Riva ME, Suyo-Vega JA, Fernández-Bedoya VH. Humanized Care From the Nurse-Patient Perspective in a Hospital Setting: A Systematic Review of Experiences Disclosed in Spanish and Portuguese Scientific Articles. Front Public Health. 2021;9:737506. https://doi.org/10.3389/fpubh.2021.737506
XReferencias
Amsrud KE, Lyberg A, Severinsson E. Development of resilience in nursing students: A systematic qualitative review and thematic synthesis. Nurse Educ Pract. 2019;41:102621. https://doi.org/10.1016/j.nepr.2019.102621
XReferencias
Bas-Sarmiento P, Fernández-Gutiérrez M, Baena-Baños M, Romero-Sánchez JM. Efficacy of empathy training in nursing students: A quasi-experimental study. Nurse Educ Today. 2017;59:59-65. https://doi.org/10.1016/j.nedt.2017.08.012
XReferencias
Taylor R, Thomas-Gregory A, Hofmeyer A. Teaching empathy and resilience to undergraduate nursing students: A call to action in the context of Covid-19. Nurse Educ Today. 2020;94:104524. https://doi.org/10.1016/j.nedt.2020.104524
XReferencias
Severino-González P, Toro-Lagos V, Santinelli-Ramos MA, Romero-Argueta J, Sarmiento-Peralta G, Kinney IS, et al. Social Responsibility and Spiritual Intelligence: University Students' Attitudes during COVID-19. Int J Environ Res Public Health. 2022;19(19):11911. https://doi.org/10.3390/ijerph191911911
XReferencias
Serpa da Fonseca RMG, Aparecida Barbosa D, Yoshikawa Egry E. Formation in Social Responsibility of Nursing Professionals: a Brazilian Perspective. Invest Educ Enferm. 2018;36(2). https://doi.org/10.17533/udea.iee.v36n2e01
Castellón-Montenegro H, Barraza-Ospino D, Borré-Ortiz YM, Lastre-Amell G, Erazo-Coronado AM, Díaz-Narváez VP. Empathy in nursing students from the Metropolitana University of Barranquilla (Colombia). Texto Contexto Enferm. 2020;29:e20180314. https://doi.org/10.1590/1980-265X-TCE-2018-0314
Ebisch SJH, Scalabrini A, Northoff G, Mucci C, Sergi MR, Saggino A, et al. Intrinsic Shapes of Empathy: Functional Brain Network Topology Encodes Intersubjective Experience and Awareness Traits. Brain Sci. 2022;12(4):477. https://doi.org/10.3390/brainsci12040477
Troncoso A, Blanco K, Rivera-Rei Á, Martínez-Pernía D. Empathy bodyssence: temporal dynamics of sensorimotor and physiological responses and the subjective experience in synchrony with the other's suffering. Front Psychol. 2024;15:1362064. https://doi.org/10.3389/fpsyg.2024.1362064
Emmerich G, Wiek J, Höfling J. Life satisfaction in patients with chronic glaucoma-An overview. Ophthalmologie. 2024;121(1):4-10. https://doi.org/10.1007/s00347-023-01925-2
Chengappa N, Rajkumar Honest PC, David K, Pricilla RA, Rahman SM, Rebecca G. Effect of BATHE interview technique on patient satisfaction in an ambulatory family medicine centre in South India. Fam Med Community Health. 2020;8(4):e000327. https://doi.org/10.1136/fmch-2020-000327
Loue S. Teaching and Practicing Humanism and Empathy through Embodied Engagement. Medicina (Kaunas). 2022;58(3):330. https://doi.org/10.3390/medicina58030330
Gonzalez-Liencres C, Shamay-Tsoory SG, Brüne M. Towards a neuroscience of empathy: ontogeny, phylogeny, brain mechanisms, context and psychopathology. Neurosci Biobehav Rev. 2013;37(8):1537-48. https://doi.org/10.1016/j.neubiorev.2013.05.001
Díaz-Narváez VP, Calzadilla-Núñez A, Alonso LM, Torres-Martínez PA, Cervantes-Mendoza M, Fajardo-Ramos E. Empathy and ontogeny: a conceptual approach. West Indian Med J. 2017;66(3):1-4. https://www.mona.uwi.edu/fms/wimj/article/3107
Kim J. Factors influencing nursing students' empathy. Korean J Med Educ. 2018;30(3):229-36. https://doi.org/10.3946/kjme.2018.97
Tang Y, Wang C, Li Q, Liu G, Song D, Quan Z, et al. Neural Network Excitation/Inhibition: A Key to Empathy and Empathy Impairment. Neuroscientist. 2024;30(6):644-65. https://doi.org/10.1177/10738584231223119
Veerareddy A, Fang H, Safari N, Xu P, Krueger F. Cognitive empathy mediates the relationship between gray matter volume size of dorsomedial prefrontal cortex and social network size: A voxel-based morphometry study. Cortex. 2023;169:279-89. https://doi.org/10.1016/j.cortex.2023.09.015
Bethlehem RAI, Seidlitz J, White SR, Vogel JW, Anderson KM, Adamson C, et al. Brain charts for the human lifespan. Nature. 2022;604(7906):525-33. https://doi.org/10.1038/s41586-022-04554-y
Maltby J, Day L, Hall S. Refining Trait Resilience: Identifying Engineering, Ecological, and Adaptive Facets from Extant Measures of Resilience. PLoS One. 2015;10(7):e0131826. https://doi.org/10.1371/journal.pone.0131826
Hojat M, DeSantis J, Shannon SC, Mortensen LH, Speicher MR, Bragan L, et al. The Jefferson Scale of Empathy: a nationwide study of measurement properties, underlying components, latent variable structure, and national norms in medical students. Adv Health Sci Educ Theory Pract. 2018;23:899-920. https://doi.org/10.1007/s10459-018-9839-9
Tzialla N, Boka V, Menexes G, Kotsanos N, Arapostathis K. Psychometric properties of the Greek version of the Jefferson Scale of Empathy and empathy levels in Greek dental postgraduate students. Eur Arch Paediatr Dent. 2023;24(6):691-70. https://link.springer.com/article/10.1007/s40368-023-00826-x
Díaz-Narváez VP, Vallecampo Contreras A, Campos de Chavarría J, Estrada-Méndez N, Sánchez de Elías DA, Vilca LW, et al. La resiliencia es un predictor de la empatía en estudiantes de Enfermería. OSFHOME 2024. https://osf.io/fahx8?view_only=71a694ddaa9247a5bee02686211ced9a
Yuan KH, Bentler PM. Three likelihoodbased methods for mean and Covariance structure analysis with nonnormal missing data. Sociol Methodol. 2000;30(1):165–200. https://doi.org/10.1111/0081-1750.00078
Rhemtulla M, Brosseau-Liard PE, Savalei V. When can categorical variables be treated as continuous? A comparison of robust continuous and categorical SEM estimation methods under suboptimal conditions. Psychol Methods. 2012;17(3):354–33. https://doi.org/10.1037/a0029315
Kline RB. Principles and Practice of Structural Equation Modeling (4th ed.). 2016. The Guilford Press.
Schumacker RE, Lomax RG. A Beginner’s Guide to Structural Equation Modeling: Fourth Edition (4th ed.). 2015. Routledge.
Cronbach LJ. Coefficient alpha and the internal structure of tests. Psychometrika. 1951;16(3):297–334. https://doi.org/10.1007/BF02310555
McDonald RP. Test Theory: A Unified Treatment. 1999. Taylor & Francis.
Viladrich C, Angulo-Brunet A, Doval E. A journey around alpha and omega to estimate internal consistency reliability. An Psicol. 2017;33(3):755–82. https://doi.org/10.6018/analesps.33.3.268401
Díaz-Narváez VP, Vallecampo Contreras A, Campos de Chavarría, Estrada-Méndez N, Sánchez de Elías DA, Vilca LW, Reyes-Reyes A, Gamarra-Moncayo J. La resiliencia, predictor de la empatía en estudiantes de Enfermería. OSFHOME. 2025. https://doi.org/10.17605/OSF.IO/AE5XH
Mylonas K, Furnham A. Bias in terms of culture and a method for reducing it: An eight-country “Explanations of Unemployment Scale” study. Educ Psychol Meas. 2014;74(1):77-96. http://dx.doi.org/10.1177/0013164413502669
Masten AS, Coatsworth JD. The development of competence in favorable and unfavorable environments. Amer Psychol. 1998;53(2):205-220. https://doi.org/10.1037/0003-066X.53.2.205
Kenner C, Boykova M. Burnout and Resilience in Neonatal Nurses. The Journal of Perinatal & Neonatal Nursing. 2023;37(3):178-180. http://dx.doi.org/10.1097/JPN.0000000000000750
Golubovich J, Chang CG, Eatough EM. Safety climate, hardiness, and musculoskeletal complaints: A mediated moderation model. Appl Ergon. 2014;45(3):757–66. https://doi.org/10.1016/j.apergo.2013.10.008
Skomorovsky A, Stevens S. Testing a Resilience Model among Canadian Forces Recruits. Mil Med. 2013;178(8):829–837. https://doi.org/10.7205/MILMED-D-12-00389
Smith BW, Dalen J, Wiggins K, Tooley E, Christopher P, Bernard J. The Brief Resilience Scale: Assessing the ability to bounce back. Int J Behav Med. 2008;15(3):194–200. https://doi.org/10.1080/10705500802222972
Howell KH, Miller-Graff LE. Protective factors associated with resilient functioning in young adulthood after childhood exposure to violence. Child Abuse Neglect. 2014;38(12):1985–94. https://doi.org/10.1016/j.chiabu.2014.10.010
Braniecka A, Trzebińska E, Dowgiert A, Wytykowska A. Mixed Emotions and Coping: The Benefits of Secondary Emotions. Plos One. 2014;9(8):e103940. https://doi.org/10.1371/journal.pone.0103940
Yuen WWY, Wong WCW, Holroyd E, Tang CSK. Resilience in Work-Related Stress among Female Sex Workers in Hong Kong. Qual Health Res. 2014;24(9):1232–41. https://doi.org/10.1177/1049732314544968
Sullivan V, Hughes V, Wilson DR. Nursing Burnout and Its Impact on Health. Nurs Clin North Am. 2022;57(1):153-69. https://doi.org/10.1016/j.cnur.2021.11.011
Rivera-Burciaga AR, Palacios M, Kemery SA. Educating for equity in palliative care: Implications of the Future of Nursing 2030 Report. J Prof Nurs. 2022;42:134-39. https://doi.org/10.1016/j.profnurs.2022.06.012
Shiraishi Y, Saito Y, Kuroki T, Yoshinaga N, Tanoue H, Hayashi Y. Research and Future Challenges for Disseminating Strengths-Based Nursing and Healthcare in Japan. Nurs Leadersh. 2024;36(4):52-56. https://doi.org/10.12927/cjnl.2024.27308
Díaz-Narváez VP, Calzadilla-Núñez A, Reyes-Reyes A, Lastre Amell G, Castellón-Montenegro H, Andrade Valles I, et al. Empathy, psychometrics, cut-off points in nursing students from Latin America. Int Nurs Rev. 2022;70(2):185-193. https://doi.org/10.1111/inr.12783
Meneses-La-Riva ME, Suyo-Vega JA, Fernández-Bedoya VH. Humanized Care From the Nurse-Patient Perspective in a Hospital Setting: A Systematic Review of Experiences Disclosed in Spanish and Portuguese Scientific Articles. Front Public Health. 2021;9:737506. https://doi.org/10.3389/fpubh.2021.737506
Tehranineshat B, Rakhshan M, Torabizadeh C, Fararouei M. Compassionate Care in Healthcare Systems: A Systematic Review. J Natl Med Assoc. 2019;111(5):546-54. https://doi.org/10.1016/j.jnma.2019.04.002
Cheraghi MA, Esmaeili M, Salsali M. Seeking Humanizing Care in Patient-Centered Care Process: A Grounded Theory Study. Holist Nurs Pract. 2017;31(6):359-368. https://doi.org/10.1097/HNP.0000000000000233
Walters DM, Maddaus M. Strategies of Well-being Training and Resilience. Thorac Surg Clin. 2024;34(3):299-308. https://doi.org/10.1016/j.thorsurg.2024.04.006
Amsrud KE, Lyberg A, Severinsson E. Development of resilience in nursing students: A systematic qualitative review and thematic synthesis. Nurse Educ Pract. 2019;41:102621. https://doi.org/10.1016/j.nepr.2019.102621
Bas-Sarmiento P, Fernández-Gutiérrez M, Baena-Baños M, Romero-Sánchez JM. Efficacy of empathy training in nursing students: A quasi-experimental study. Nurse Educ Today. 2017;59:59-65. https://doi.org/10.1016/j.nedt.2017.08.012
Roberts ML, Kaur T. Effect of Storytelling and Empathy Training to Support Affective Learning in Undergraduate Nursing Students. Nurse Educ. 2023;48(5):260-64. https://doi.org/10.1097/NNE.0000000000001419
Taylor R, Thomas-Gregory A, Hofmeyer A. Teaching empathy and resilience to undergraduate nursing students: A call to action in the context of Covid-19. Nurse Educ Today. 2020;94:104524. https://doi.org/10.1016/j.nedt.2020.104524
Severino-González P, Toro-Lagos V, Santinelli-Ramos MA, Romero-Argueta J, Sarmiento-Peralta G, Kinney IS, et al. Social Responsibility and Spiritual Intelligence: University Students' Attitudes during COVID-19. Int J Environ Res Public Health. 2022;19(19):11911. https://doi.org/10.3390/ijerph191911911
Serpa da Fonseca RMG, Aparecida Barbosa D, Yoshikawa Egry E. Formation in Social Responsibility of Nursing Professionals: a Brazilian Perspective. Invest Educ Enferm. 2018;36(2). https://doi.org/10.17533/udea.iee.v36n2e01