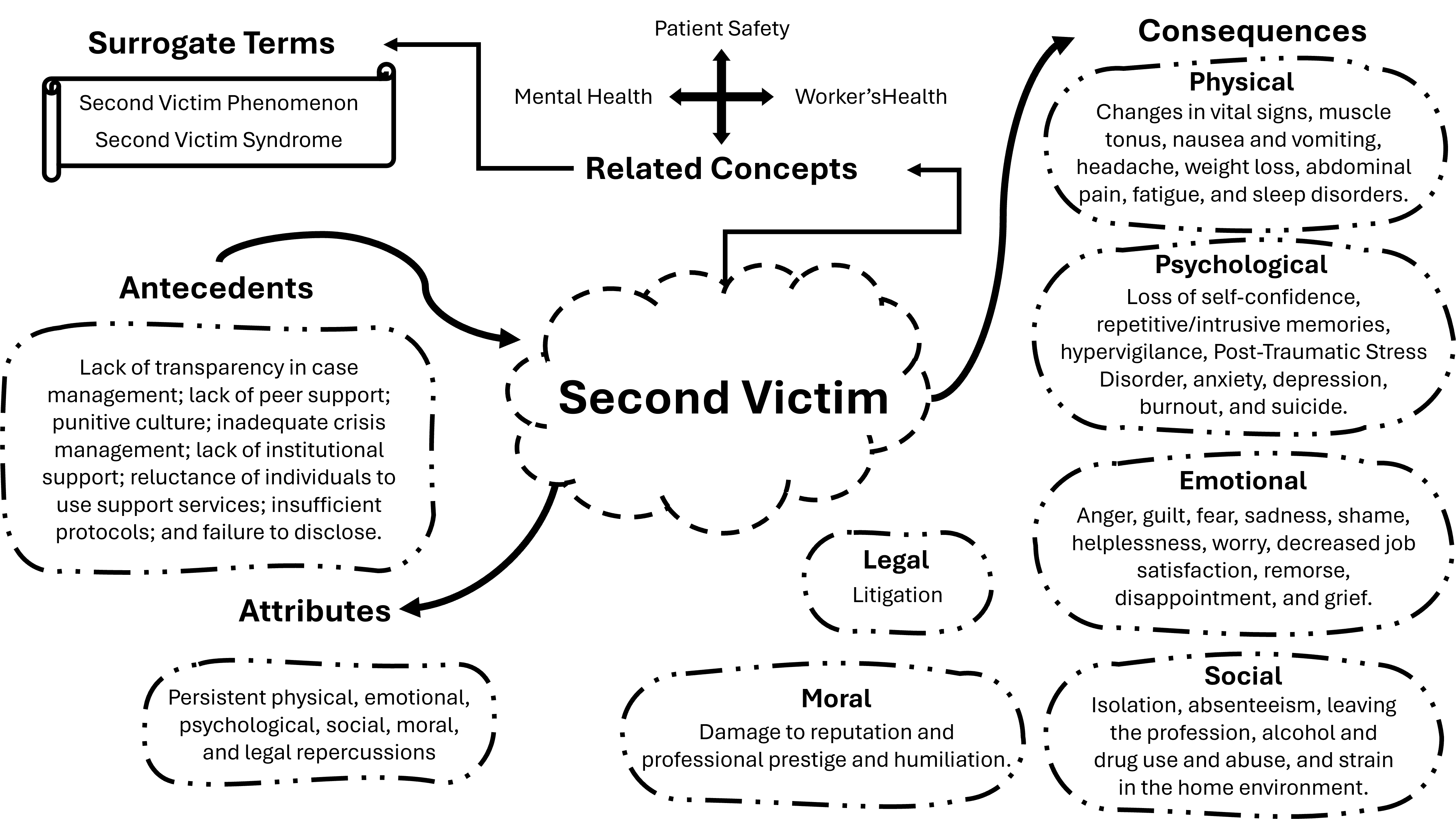
Figure 2. Conceptual structure of the second victim concept and its relationships among
antecedents, attributes, consequences, and related concepts, Fortaleza, Ceará, 2024
3. Identification of a model case for the concept
In this analysis, a real case reported in the literature was used, with the appropriate
adaptations to
protect the identity of those involved. The selected practical example illustrates the
“second
victim”
concept, highlighting its key attributes and consequences. This case aims to highlight the
concept's
characteristics, provide an accurate understanding, and facilitate its application.
“An experienced pediatric intensive care nurse, recognized for her
dedication,
made a medication
error by administering an excessive dose of calcium chloride to an infant with severe heart
problems.
The error occurred due to a momentary distraction during medication preparation. Although
she
promptly recognized the error, reported the incident, and intervened to stabilize the
patient,
she was
overwhelmed by intense feelings of guilt and remorse for having caused harm to the infant,
who
died
five days later. It is believed that the error exacerbated the child's heart condition,
contributing to the
fatal outcome.
The case received widespread media coverage, prompting the nursing board to
initiate an
investigation.
During the proceedings, the institution placed the nurse on administrative leave without
providing
adequate emotional or professional support. In the absence of peer support, she began to
question
her professional competence, feeling deeply frustrated, ashamed, and helpless.
After the investigation was completed, the institution terminated her
employment
contract, and
the
nursing board imposed sanctions, including a fine and a four-year probationary period during
which
her medication administration would be supervised. The public repercussions and professional
consequences further aggravated her emotional state, leading to insomnia, anxiety, and
severe
depression. She began to repeatedly relive the incident in her thoughts and dreams,
progressively
withdrawing from friends, family, and her religious community.
Despite several attempts to re-enter the workforce, the nurse encountered
barriers, which
intensified
her isolation and despair. Faced with the prospect of no longer being able to practice her
profession,
persistent sadness and feelings of inadequacy culminated in her decision to take her own
life
seven
months after the incident. The impact of her death was profound, with former patients and
their
family members attending a memorial service in her honor, where they expressed gratitude for
her
compassion and dedication throughout her career.”
4. Hypotheses identification and their implications
The analysis of the “second victim” concept based on Rodgers’ evolutionary approach offers a
broader
and more practical understanding of the construct. This proposal enables the integration of
the
concept into discussions on patient safety and workers’ health.
However, studies on second victims have examined the experiences and
perceptions of formally
trained healthcare professionals. Future research on the topic should adopt a broader scope.
The
conceptual framework proposed in this research underscores the need to include other
healthcare
workers who are indirectly involved in care, share responsibility for patient safety, and
may
also be
affected as “second victims.”
It is also important to emphasize the need for future studies that
differentiate
between the
“second
victim phenomenon” and “second victim syndrome.” These terms are often used interchangeably
with “second victim,” yet they lack a precise conceptual definition.
Discussion
Concept contributions
The “second victim” concept presented in this study revisits and expands the understanding
of
this
condition by incorporating new dimensions into its definition. The proposal’s distinguishing
feature is
its comprehensive approach, which includes not only physicians but all healthcare workers,
scholars,
and administrative or support staff as potentially affected individuals. The definition also
encompasses
the physical, emotional, psychological, social, ethical, and legal consequences these
individuals experience,
highlighting the need for timely support to prevent chronic effects and associated diseases.
The inclusion of other healthcare workers, such as nurses, physical
therapists, and pharmacists, as well
as other non-traditional healthcare roles, such as laboratory technicians, cleaning
staff45,
radiotherapy
professionals, and porters17, in addition to practicum
students30,31,35,36,40,49
,
represents a step forward in
understanding the vulnerability of these groups. However, many of these professionals were
generically
classified as “others” in the studies, highlighting the need for greater recognition and formal
inclusion of
these groups in discussions on patient safety and exposure to events that may render them potential
second victims.
The recognition that other professional categories, whether in training or indirectly
involved in
patient
care, can also become second victims represents a significant contribution. This finding is a
crucial
step
toward ensuring that educational institutions and hospitals develop more comprehensive support
programs, so that no individual, regardless of their role or career status, is left without support
in
times
of crisis.
The incorporation of repercussions and consequences into the definition, in turn,
supports the
conclusion that the resulting harm also affects healthcare workers. Such recognition is essential
for
planning practical approaches to support these professionals and promote actions that facilitate
their
recovery and prevent future adverse effects. A systematic review with meta-analysis revealed that
the
second victim syndrome affects 58% of professionals over the course of their careers, of whom 60%
recover within one month, while 20% take more than a year to recover or do not recover50
Thus, including appropriate and timely support as an essential component of managing
these
experiences and recognizing its critical role in preventing progression toward chronic and
pathological
responses serves as a warning and holds health institutions accountable for developing support
strategies for professionals to prevent these unfavorable outcomes.
Support mechanisms must be accessible, structured, and widely disseminated to ensure
positive
outcomes and encourage constructive approaches to addressing second victims’ experiences41. In
this context, organizational culture directly influences the suffering of these professionals and
may
either mitigate or intensify it. Punitive environments exacerbate adverse effects, undermine a
culture
of patient safety, promote the concealment of errors, and increase underreporting, thereby hindering
organizational learning and the correction of failures.40
Contextual basis
The concept’s antecedents highlight how a weakened patient safety culture contributes to the
negative
impacts on second victims. Punitive organizational cultures exacerbate emotional symptoms. These
cultures, characterized by blame and fear-based management, compromise professional performance
and hinder efforts to prevent new adverse events51. Therefore, promoting a patient safety culture
based
on transparency, without blaming or punishment, and continuous learning is essential for advancing
organizational improvements48.
The attributes identified as essential to the concept reflect the prolonged and
multidimensional
nature of the experience, encompassing physical, emotional, psychological, social, moral, and legal
repercussions, and highlighting the depth of its impact. The manifestations are particular and
affect
social, cultural, emotional, spiritual, and physical areas52.
Recurrent symptoms, such as hypervigilance, flashbacks,
and feelings of shame, may persist for months
or even years, especially in the absence of adequate institutional support5. When left untreated,
these symptoms may progress to severe conditions, such as post-traumatic stress disorder, anxiety,
depression, and suicidal ideation53.
Although some individuals recover in the short term, others
experience manifestations that may last a lifetime17, underscoring the need for effective
interventions
to prevent chronicity and worsening outcomes.
The discussion of duration, chronicity, and progression toward pathological responses
in
the
second
victim condition is intertwined with the surrogate terms identified in the analyzed studies. The
expressions “second victim phenomenon”21,26,
33,35,
38,45,
46,49
and “second victim syndrome”13, 18, 30 are often
used interchangeably with “second victim.” However, based on the literature reviewed, these terms
are
more related to lived experiences than to the individuals themselves. Nevertheless, these
expressions
reflect different aspects: “phenomenon” refers to the symptomatic manifestations following the
incident, whereas “syndrome” is associated with cases in which the professional develops a
pathological
condition due to a lack of resources to cope with the experience.
The second victim condition is closely related to other important concepts, such as
mental
health,
workers’ health, and patient safety, as extensively discussed in the study. These areas converge in
addressing worker well-being, highlighting the importance of preventive and supportive measures
in situations of work-related trauma. The relationship between occupational health and patient
safety
has gained attention, as adequate working conditions directly influence the quality of care and
patient
safety1.
Ensuring service quality requires continuous investment in education, training, and
the
maintenance
of professionals’ health. However, high rates of illness among workers reveal a concerning reality,
exacerbated by the absence of institutional policies aimed at balancing worker safety and patient
safety. This scenario highlights the importance of implementing integrated actions that ensure this
essential combination: safe workers and safe patients54.
Critical analysis of the concept
The analysis of the manuscripts included in this study indicates that, although the “second
victim”
concept has become established over time, its use remains controversial. Concerns have been raised
abput the appropriateness of using the term “victim” to describe healthcare workers, as it may
convey
an idea of passivity, imply exemption from responsibility, and minimize the need for ethical and
professional accountability.
Critics of the term “second victim” argue that it may conflict with patient safety
culture,
divert attention
from the needs of affected patients and their families, and place excessive emphasis on
professionals at
the expense of a balanced approach24.
According to them, the terminology may minimize or undermine
patients’ experience by suggesting that “everyone is a victim,” thereby diluting the real pain
experienced
by patients and their families.
In addition, critics point out that this expression may convey the perception that
professionals
are
more concerned with themselves than with their patients. For this reason, some researchers advocate
reevaluating and, if necessary, replacing the term with more appropriate alternatives developed in
consultation with patients and professionals39.
By contrast, proponents of the term “second victim” argue that it reflects the
reality of
professionals
affected by errors arising from flawed systems, highlighting the need for institutional support and
an
approach focused on organizational well-being. The term is also seen as raising institutional
awareness
and promoting a patient safety culture that includes support for workers as an essential component
of
learning and prevention strategies25.
Supporters contend that introducing the term has been beneficial, as it has brought
attention to
the impact of errors on healthcare professionals without diminishing patients’ experiences. They
emphasize that, although patient-centered care is essential, the well-being of professionals is
equally
crucial to the safety and quality of care. They further argue that the focus should be on preventing
new
incidents through collaboration among patients, family members, and professionals, moving beyond
terminological debates and prioritizing practical support and prevention strategies.27
The creator of the term, Albert Wu, acknowledges that, despite criticism, the concept
is
well
established
and understood among healthcare professionals, and that changing it could lead to confusion. He
argues
that the term serves its purpose of drawing attention to the problems professionals face. However,
he
also admits that there are valid arguments both in favor and against its use. In this regard, he
suggests
that, at present, it is essential to allow advocates to adopt the terminology with which they feel
most
comfortable, provided that the goal remains the recognition of the problem and the implementation
of appropriate solutions29.
The objective of this study was to conduct a concept analysis of the term “second
victim”
with
the aim
of establishing a more precise definition of the individuals involved and the repercussions of
adverse
events on healthcare workers. The study does not seek to reformulate the existing terminology;
however, it acknowledges that the term “second victim” may not be the most appropriate for referring
to these professionals. Accordingly, there is a need for further studies to propose alternative,
equally
representative terminologies that preserve the impact and relevance of the current term, while
promoting greater precision and acceptance in academic and practical fields.
As a concept analysis, this study has limitations. Although it provides a historical
and
dynamic
contextualization of the concept, it relies on the researchers’ interpretations, which may introduce
bias
and limit the generalizability of its propositions. Furthermore, the decision to include only
open-access
articles may have limited the sample analyzed, excluding relevant studies available in
restricted-access
databases. Nevertheless, the study contributes to the conceptual development and definition of the
concept and may inform future research. In this sense, further research is recommended to integrate
approaches that strengthen the practical application of the concept.
Conclusions
The concept analysis based on Rodgers’ evolutionary model provided a more accurate
understanding
of the “second victim” concept, with relevant implications for patient safety. Accordingly, the
“second
victim” concept refers to healthcare workers, scholars, and administrative or support staff who are
directly or indirectly involved in patient care and who, following an unintentional
healthcare-related
incident, experience physical, emotional, and psychological reactions with repercussions across the
biopsychosocial, ethical, and legal dimensions. Without appropriate and timely support, these
reactions
may become chronic and, eventually, pathological.
The identified antecedents indicate that weaknesses in patient safety culture and the
absence of
support
mechanisms favor the emergence of the second victim condition among healthcare professionals. The
influence of historical and cultural factors contributes to the perpetuation of suffering,
reinforcing
reluctance to seek help and maintaining an image of perfection in healthcare. In this context, the
second victim experience warrants reflection on the physical, emotional, and psychological reactions
that characterize it and underscore the need for appropriate support.
The consequences of this condition affect both professionals’ well-being and patient
safety, as
well
as organizational dynamics, compromising the quality of care and workers’ performance. Accordingly,
concepts related to the “second victim” are intrinsically linked to patient safety and workers’
health,
highlighting the need for effective institutional approaches to prevention and support to minimize
its
negative effects and promote a safer and more supportive work environment.
Conflict of interest: The authors declare no conflicts of interest.
Funding: The research received no funding.
Author Contributions: Matheus Tavares França da Silva:
Conceptualization; Data
curation;
Formal Analysis; Investigation; Methodology; Project administration; Software; Writing -
original draft. Caroliny Cristine dos Santos Mendes: Data curation ; Formal Analysis; Methodology;
Project administration; Software. Rebeca Furtado Fernandes: Data curation; Formal Analysis;
Methodology; Project administration; Software. Sherida Karanini Paz de Oliveira: Supervision;
Validation; Writing – revision & editing. Rhanna Emanuela Fontenele Lima de Carvalho: Supervision;
Validation; Writing – revision & editing.
References
-
World Health Organization. Global patient safety action plan
2021–2030:
towards eliminating
avoidable harm in health care. Geneva: WHO. [Internet] 2021 [cited 2024 Jul 5]. Available
from:
https://www.conass.org.br/wp-content/uploads/2024/07/9789240095458-eng.pdf
-
World Health Organization. Global patient safety report
2024.
Geneva:
WHO. [Internet] 2024
[cited 2024 Jul 6]. Available from:
https://iris.who.int/handle/10665/376928
-
Wu AW.
Medical error: the second victim. The doctor who makes the mistake needs help too.
BMJ.
2000;320(7237):726-7.
https://doi.org/10.1136/bmj.320.7237.726
-
Yorkshire Quality and Safety Research Group (Bradford Institute for
Health Research and University of Leeds) and the Yorkshire and Humber Improvement
Academy (YHIA).
Spotlight on the ‘Second Victim’ term. Just Culture Network. [Internet] 2022 [cited 2024 Jul
8].
Available from:
https://secondvictim.co.uk/wp-content/uploads/2022/07/JCN-branded-Full-Spotlight-SV-piece-v4.pdf
-
Vanhaecht K, Seys D, Russotto S, Strametz R, Mira J,
Sigurgeirsdóttir S,
et
al. An Evidence
and Consensus-Based Definition of Second Victim: A Strategic Topic in Healthcare Quality,
Patient
Safety, Person-Centeredness and Human Resource Management. Int J Environ Res Public
Health.
2022;19(24):16869. https://doi.org/10.3390/ijerph192416869
-
Rodgers BL. Concept Analysis: An Evolutionary View. In:
Rodgers
BL,
Knafl KA, eds. Concept
Development in Nursing - Foundations, Techniques, and Applications. 2nd ed. Philadelphia:
Saunders; 2000.
-
Peters MDJ, Godfrey C, McInerney P, Munn Z, Tricco AC, Khalil,
H.Scoping Reviews (2020).
Aromataris E, Lockwood C, Porritt K, Pilla B, Jordan Z, editors. JBI Manual for Evidence
Synthesis
JBI. 2024:417-462. https://doi.org/10.46658/JBIMES-24-09
-
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD,
et
al. The PRISMA 2020
statement: an updated guideline for reporting systematic. Rev Panam Salud Publica.
2022;46:e112. https://doi.org/10.26633/RPSP.2022.112
-
Da Silva MTF, Fernandes RF, Mendes CCS, Oliveira SKP, Carvalho
REFL.
Atributos, Antecedentes
e Consequentes do Conceito de Segunda Vítima em Trabalhadores da Saúde: Revisão de Escopo.
OSF;
2025.
https://doi.org/10.17605/OSF.IO/T8UCF
-
Silva MTF da; Mendes CCS; Fernandes, RF; Oliveira, SKP; Anjos, SJSB;
Carvalho,
RFL. Segunda
Vítima: Análise de Conceito Fundamentada no Modelo Evolucionário de Rodgers”,Mendeley
Data,
2025. V1. https://doi.org/10.17632/7mrmv8p4vv.1
-
Scott SD, Hirschinger LE, Cox KR, McCoig M, Brandt J, Hall LW.
The
natural history of recovery
for the healthcare provider "second victim" after adverse patient events. Qual Saf
Health Care.
2009;18(5):325-30. https://doi.org/10.1136/qshc.2009.032870
-
Edrees HH, Paine LA, Feroli ER, Wu AW. Health care workers
as second
victims of medical errors.
Pol Arch Med Wewn. 2011;121(4):101-8. https://dx.doi.org/10.20452/pamw.1033
-
Clancy CM. Alleviating "second victim" syndrome: how we
should handle
patient harm. J Nurs
Care Qual. 2012;27(1):1-5. https://dx.doi.org/10.1097/NCQ.0b013e3182366b53
-
Hall LW, Scott SD.
The second victim of adverse health care events.
Nurs Clin North Am.
2012;47(3):383-93. https://dx.doi.org/10.1016/j.cnur.2012.05.008
-
Schiechtl B, Hunger MS, Schwappach DL, Schmidt CE, Padosch
SA. Second victim: Critical
incident stress management in clinical medicine. Anaesthesist. 2013;62:734-41. https://dx.doi.org/10.1007/s00101-013-2215-5
-
Harrison R, Lawton R, Perlo J, Gardner P, Armitage G, Shapiro
J.
Emotion and Coping in the
Aftermath of Medical Error: A Cross-Country Exploration. Journal of Patient Safety,
2015,11(1):28-
35. https://dx.doi.org/10.1097/PTS.0b013e3182979b6f
-
Mira JJ, Carrillo I, Lorenzo S, Ferrús L, Silvestre C, Pérez-Pérez
P, et
al. The aftermath of adverse
events in Spanish primary care and hospital health professionals.
BMC Health Serv Res. 2015,15:151.
https://dx.doi.org/10.1186/s12913-015-0790-7
-
Marmon LM, Heiss K. Improving surgeon wellness: The second
victim
syndrome and quality of
care.
Semin Pediatr Surg. 2015;24(6):315-318. https://dx.doi.org/10.1053/j.sempedsurg.2015.08.011
-
Rinaldi C, Leigheb F, Vanhaecht K, Donnarumma C, Panella M.
Becoming a
"second victim"
in health care: Pathway of recovery after adverse event. Rev Calid Asist.
2016;31(2):11-9. https://dx.doi.org/10.1016/j.cali.2016.05.001
-
Van Gerven E, Vander Elst T, Vandenbroeck S, Dierickx S, Euwema M,
Sermeus W, et
al. Increased Risk of Burnout for Physicians and Nurses Involved in a Patient
Safety
Incident. Med
Care. 2016;54(10):937-43. https://dx.doi.org/10.1097/MLR.0000000000000582
-
Quillivan RR, Burlison JD, Browne EK, Scott SD, Hoffman JM.
Patient
Safety Culture and the
Second Victim Phenomenon: Connecting Culture to Staff Distress in Nurses.
Jt Comm J Qual Patient
Saf.
2016;42(8):377-384. https://dx.doi.org/10.1016/s1553-7250(16)42053-2
-
Han K, Bohnen JD, Peponis T, Martinez M, Nandan A, Yeh DD, et
al. The
Surgeon as the Second
Victim? Results of the Boston Intraoperative Adverse Events Surgeons' Attitude (BISA) Study.
J Am
Coll Surg. 2017;224(6):1048-1056. https://dx.doi.org/10.1016/j.jamcollsurg.2016.12.039
-
Van Gerven E, Deweer D, Scott SD, Panella M, Euwema M, Sermeus W et
al.
Personal, situational
and organizational aspects that influence the impact of patient safety incidents: A
qualitative
study. Rev Calid Asist.
2016;31(2):34-46. https://dx.doi.org/10.1016/j.cali.2016.02.003
-
Clarkson MD, Haskell H, Hemmelgarn C, Skolnik P J. Abandon
the term
“second victim”.
BMJ.
2019;364:l1233. https://dx.doi.org/10.1136/bmj.l1233
-
Petersen IG. The term “second victim” is appropriate for
frontline
Workers.
BMJ.
2019;365:l2157 https://dx.doi.org/10.1136/bmj.l2157
-
Kobe C, Blouin S, Moltzan C, Koul R. The Second Victim
Phenomenon:
Perspective of Canadian Radiation Therapists.
J Med Imaging Radiat Sci. 2019;50(1):87-97.
https://dx.doi.org/10.1016/j.jmir.2018.07.004
-
Gómez-Durán EL, Tolchinsky G, Martin-Fumadó C, Arimany-Manso
J.
Neglecting the "second
victim" will not help harmed patients or improve patient safety.
BMJ. 2019;365:l2167. https://dx.doi.org/10.1136/bmj.l2167
-
Gupta K, Lisker S, Rivadeneira NA, Mangurian C, Linos E, Sarkar U.
Decisions and repercussions
of second victim experiences for mothers in medicine (SAVE DR MoM). BMJ. Qual Saf.
2019;28(7):564-
573. https://dx.doi.org/10.1136/bmjqs-2018-008372
-
Wu AW, Shapiro J, Harrison R, Scott SD, Connors C, Kenney L, et al.
The Impact of Adverse
Events on Clinicians: What's in a Name?. J Patient Saf.
2020;16(1):65-72. https://dx.doi.org/10.1097/PTS.0000000000000256
-
Donahue KR, Gossai T, Succar L, Bhakta SB, Varkey AC.
Second victim
syndrome and
the pharmacy learner. J Am Pharm Assoc. 2020;60(4):e14-e17. https://dx.doi.org/10.1016/j.
japh.2020.01.020
-
Huang H, Chen J, Xiao M, Cao S, Zhao Q. Experiences and
responses of
nursing students as
second victims of patient safety incidents in a clinical setting: A mixed-methods study.
J Nurs
Manag.
2020;28(6):1317-1325. https://dx.doi.org/10.1111/jonm.13085
-
Choi EY, Pyo J, Lee W, Jang SG, Park YK, Ock M, et al.
Nurses'
experiences of patient safety
incidents in Korea: a cross-sectional study. BMJ Open.
2020;10(10):e037741. https://dx.doi.org/10.1136/bmjopen-2020-037741
-
Burlison JD, Quillivan RR, Scott SD, Johnson S, Hoffman JM.
The
Effects of the Second
Victim Phenomenon on Work-Related Outcomes: Connecting Self-Reported Caregiver Distress
to Turnover Intentions and Absenteeism. J Patient Saf.
2021;17(3):195-199. https://dx.doi.org/10.1097/PTS.0000000000000301
-
Almeida PP. Avaliação dos profissionais de enfermagem
sobre a cultura
de segurança e as
manifestações de segunda vítima de evento adverso. 2021. 83 f. Dissertação [Mestrado
Profissional
em Saúde Ambiental e Saúde do Trabalhador] - Universidade Federal de Uberlândia, Uberlândia,
2021. http://doi.org/10.14393/ufu.di.2021.556
-
Choi EY, Pyo J, Ock M, Lee H. Second victim phenomenon
after patient
safety incidents among
Korean nursing students: A cross-sectional study. Nurse Educ Today.
2021;107:105115. https://dx.doi.org/10.1016/j.nedt.2021.105115
-
Van Slambrouck L, Verschueren R, Seys D, Bruyneel L, Panella M,
Vanhaecht K.
Second
victims among baccalaureate nursing students in the aftermath of a patient safety incident:
An exploratory cross-sectional study. J Prof Nurs.
2021;37(4):765-770. https://dx.doi.org/10.1016/j.profnurs.2021.04.010
-
Fatima S, Soria S, Esteban-Cruciani N. Medical errors
during training:
how do residents cope? abdescriptive study. BMC Med Educ.
2021;21(1):408. https://dx.doi.org/10.1186/s12909-021-02850-1
-
Magaldi M, Perdomo JM, López-Baamonde M, Chanzá M, Sanchez D, Gomar
C.
Second victim
phenomenon in a surgical area: online survey.
Rev Esp Anestesiol Reanim.
2021;68(9):504-512. https://dx.doi.org/10.1016/j.redar.2020.11.009
-
Tumelty ME. The Second Victim: A Contested Term?
J Patient Saf. 2021;17(8):e1488-e1493.
https://dx.doi.org/10.1097/PTS.0000000000000558
-
Tavares APM, Barlem JGT, Silveira RS da, Dalmolin G de L, Feijó G
dos S, Machado
IA, et al. Support provided to nursing students in the face of patient safety
incidents: a
qualitative study.
Rev Bras Enferm.
2022;75(2):e20220009. https://doi.org/10.1590/0034-7167-2022-0009pt
-
Quadros DV de, Magalhães AMM de, Wachs P, Severo IM, Tavares JP, Dal
Pai D.
Modelagem de
quedas de pacientes adultos e as repercussões à Enfermagem como segunda vítima. Rev
Latino-
Am Enfermagem.
2022;30:e3617. https://doi.org/10.1590/1518-8345.5830.3617
-
Ganahl S, Knaus M, Wiesenhuetter I, Klemm V, Jabinger EM, Strametz
R.
Second Victims
in Intensive Care-Emotional Stress and Traumatization of Intensive Care Nurses in Western
Austria after Adverse Events during the Treatment of Patients.
Int J Environ Res Public Health.
2022;19(6):3611. https://doi.org/10.3390/ijerph19063611
-
Flórez F, López L, Bernal C. Prevalencia de eventos
adversos y sus
manifestaciones en
profesionales de la salud como segundas víctimas. Biomed. 2022; 42(1):184-195.
https://doi.org/10.7705/biomedica.6169
-
Quadros DV de , Magalhães AMM de, Boufleuer E, Tavares JP,
Kuchenbecker R de S,
Dal Pai D. Falls Suffered by Hospitalized Adult Patients: Support to the
Nursing Team as
the Second Victim.
Aquichan.
2022;22(4):e2246. https://doi.org/10.5294/aqui.2022.22.4.6
-
Krommer E, Ablöscher M, Klemm V, Gatterer C, Rösner H, Strametz R,
et al.
Second Victim
Phenomenon in an Austrian Hospital before the Implementation of the Systematic Collegial
Help Program KoHi: A Descriptive Study. Int J Environ Res Public Health.
2023;20(3):1913. https://doi.org/10.3390/ijerph20031913
-
Mousa O, Sadeq Alghazal M, Abdullah AlBather A, Nasser Alhassan A,
Hussain
Alamer M,
Taher Alghadeer Z et al. A Study on Patient Safety Incidents and the Second
Victim Phenomenon
Among Healthcare Providers in Al-Ahsa, Saudi Arabia. Cureus. 2023;15(11):e49324.
https://doi.org/10.7759/cureus.49324
-
Silveira SE da, Tomaschewski-Barlem JG, Tavares APM, Paloski G do R,
Feijó G dos
S, Cabral CN. Impactos de incidentes de segurança do paciente na enfermagem:
um olhar para
a segunda
vítima. Rev enferm UERJ.
2023;31(1):e73147. https://doi.org/10.12957/reuerj.2023.73147
-
Alevi JO, Draganov PB, Gonçalves GCS, Zimmermann GS, Giunta L, Mira
JJ, et al.
O enfermeiro recém-formado na condição de segunda vítima. Acta paul enferm.
2024;37:eAPE02721.
https://doi.org/10.37689/acta-ape/2024AO0002721
-
Albert-Galbis A, Pérez-Cañaveras RM, Vaismoradi M, Vizcaya-Moreno
MF.
The second victim phenomenon: A qualitative study among bachelor's degree nursing students
within
the clinical learning environment. Nurse Educ Pract. 2024;78:104038.
https://doi.org/10.1016/j.nepr.2024.104038
-
Naya K, Aikawa G, Ouchi A, Ikeda M, Fukushima A, Yamada S, et al.
Second victim syndrome in
intensive care unit healthcare workers: A systematic review and meta-analysis on types,
prevalence, risk factors, and recovery time. PLoS One. 2023;18(10):e0292108.
https://doi.org/10.1371/journal.pone.0292108
-
Lemos G de C, Azevedo C, Bernardes MFVG, Ribeiro HCTC, Menezes AC,
Mata LRF da.
A Cultura
de Segurança do Paciente no Âmbito da Enfermagem: Reflexão Teórica. Revista de
Enfermagem do
Centro-Oeste Mineiro.
2018;8:e2600. https://doi.org/10.19175/recom.v8i0.2600
-
Ozeke O, Ozeke V, Coskun O, Budakoglu II. Second victims
in health
care: current perspectives.
Adv Med Educ Pract.
2019;10:593-603. https://doi.org/10.2147/AMEP.S185912
-
Busch IM, Moretti F, Purgato M, Barbui C, Wu AW, Rimondini M.
Psychological and Psychosomatic
Symptoms of Second Victims of Adverse Events: a Systematic Review and Meta-Analysis.
J Patient
Saf.
2020;16(2):e61-e74. https://doi.org/10.1097/PTS.0000000000000589
-
Baldonedo-Mosteiro M, Almeida MC dos S, Baptista PCP,
Sánchez-Zaballos M,
Rodriguez-
Diaz FJ, Mosteiro-Diaz MP. Burnout syndrome in Brazilian and Spanish nursing
workers.
Rev
Latino-Am Enfermagem.
2019;27:e3192. https://doi.org/10.1590/1518-8345.2818.3192