Abstract
Introduction: Malnutrition is common in cardiac surgery patients and
it´s associated with adverse
clinical outcomes. However, there are no validated criteria for the nutritional diagnosis in this
population.
Objective: To determine the criterion validity and inter-rater reliability of the GLIM
criteria for the
diagnosis of malnutrition and the prediction of outcomes in cardiac surgery. Materials and
Methods: Validation study in adults scheduled for cardiac surgery. Concurrent validity was
established with the
Subjective Global Assessment and the predictive validity with 30-day hospital readmission. Reliability
was assessed with two professionals. The analyses and cut-off points of the GLIM validation guide were
followed. Statistical processing was performed in R and Jamovi.
Results:
Inter-rater reliability of GLIM
was demonstrated, with almost perfect agreement (Kappa 0.94, 95% CI 0.88-0.99, p<0.001), as well as its
predictive validity for hospital readmission (RRa 2.59, 95% CI 1.09 - 7.02, p 0.04). Thresholds for
concurrent validity were not met (sensitivity 88.0%, CI 95% 68.8-97.5%; specificity 76.9%, CI 95%
56.4- 91.0%). Discussion: The lack of concurrent validity may be explained by
differences in muscle mass
estimation between diagnostic methods. The results are consistent with previous literature
supporting
the reliability and predictive ability of GLIM.
Conclusion:
GLIM criteria are reliable and predict relevant
outcomes in cardiac surgery, supporting their usefulness for nutritional diagnosis and their
potential
application in the early identification of patients eligible for preoperative optimization
interventions.
Keywords: Protein-Energy Malnutrition; Cardiac Surgical
Procedures; Validation Study; Enhanced
Recovery After Surgery; Reproducibility of Results.
Resumen
Introducción: La desnutrición es frecuente en pacientes de cirugía
cardiaca y se asocia con desenlaces clínicos adversos. Sin embargo,
no existen criterios validados para el diagnóstico nutricional de esta
población.
Objetivo: Determinar la validez de criterio y la confiabilidad
interevaluador de los criterios GLIM para el diagnóstico de desnutrición
y la predicción de desenlaces en cirugía cardiaca. Materiales y Métodos: Estudio de
validación en adultos programados para cirugía
cardiaca. La validez concurrente se estableció con la Valoración Global
Subjetiva y la validez predictiva con el reingreso hospitalario a 30
días. La confiabilidad se evaluó con dos profesionales. Se siguieron
los análisis y puntos de corte de la guía de validación de GLIM. El
procesamiento estadístico se efectuó en R y Jamovi. Resultados:
Se
demostró la confiabilidad interevaluador de GLIM, con concordancia
casi perfecta (Kappa 0,94, IC 95% 0,88-0,99, p<0,001), y su validez predictiva para reingreso
hospitalario (RRa 2,59, IC 95% 1,09 – 7,02, p 0,04). No se alcanzaron los umbrales de validación
concurrente (sensibilidad 88,0%, IC 95% 68,8-97,5%; especificidad 76,9%, IC 95% 56,4-91,0%).
Discusión: La falta de validación concurrente podría
explicarse por diferencias en la estimación de la masa muscular
entre métodos diagnósticos. Los resultados coinciden con literatura
previa que respalda la confiabilidad y capacidad predictiva de GLIM. Conclusión:
Los criterios GLIM son confiables y predicen desenlaces
relevantes en cirugía cardiaca, lo que respalda su utilidad para el
diagnóstico nutricional y su potencial aplicación en la identificación
temprana de pacientes candidatos a intervenciones de optimización
preoperatoria.
Palabras Clave: Desnutrición Proteico-Calórica; Procedimientos
Quirúrgicos Cardíacos; Estudio de Validación; Recuperación Mejorada
Después de la Cirugía; Reproducibilidad de los Resultados.
Resumo
Introdução: A desnutrição é frequente em pacientes submetidos à cirurgia
cardíaca e está associada a desfechos clínicos adversos. No entanto, não existem critérios validados
para o diagnóstico nutricional
nessa população.
Objetivo: Determinar a validade de critério e a confiabilidade entre avaliadores dos
critérios GLIM para o diagnóstico de desnutrição e a predição de desfechos em cirurgia cardíaca.
Materiais e
Métodos:
Estudo de validação realizado em adultos candidatos à cirurgia cardíaca. A validade concorrente
foi estabelecida com a Avaliação Global Subjetiva e a validade preditiva com a readmissão hospitalar em
30 dias. A confiabilidade foi avaliada por dois profissionais. As análises e pontos de corte seguiram o
guia
de validação dos critérios GLIM. O processamento estatístico foi realizado nos programas R e Jamovi.
Resultados: Demonstrou-se a confiabilidade entre avaliadores dos critérios GLIM, com
concordância quase
perfeita (Kappa 0,94, IC 95% 0,88–0,99, p<0,001), e sua validade preditiva para readmissão hospitalar
(RRa 2,59, IC 95% 1,09–7,02, p 0,04). Não foram alcançados os limiares de validade concorrente
(sensibilidade 88,0%, IC 95% 68,8–97,5%; especificidade 76,9%, IC 95% 56,4–91,0%).
Discussão: A ausência de validade
concorrente pode ser explicada por diferenças na estimativa da massa muscular entre métodos
diagnósticos.
Os resultados são consistentes com a literatura prévia que respalda a confiabilidade e a capacidade
preditiva dos critérios GLIM.
Conclusão: Os critérios GLIM são confiáveis e predizem desfechos relevantes em
cirurgia cardíaca, apoiando sua utilidade para o diagnóstico nutricional e seu potencial na
identificação
precoce de pacientes candidatos a intervenções de otimização pré-operatória.
Palavras-Chave: Desnutrição Proteico-Calórica; Procedimentos
Cirúrgicos Cardíacos; Estudo de Validação;
Recuperação Pós-Cirúrgica Melhorada; Reprodutibilidade dos Testes.
Introduction
Disease-related malnutrition
Malnutrition is defined as an imbalance between the formation and breakdown of body tissues
and nutrient reserves, leading to loss of muscle and organ mass, decreased physical and mental
function, and unfavorable clinical outcomes1
. In particular, disease-related malnutrition (DRM) results
from reduced nutrient intake or absorption caused by acute or chronic diseases, with or without an
associated systemic inflammatory response2. Its average global prevalence is estimated at
30.9%3 and in Latin America,
prevalences ranging from 40% to 60% have been reported in hospital settings4. DGiven its magnitude and relevance, the World Health
Organization (WHO) recently approved codes
5B72.0 and 5B72.1 in the International Classification of Diseases, 11th Revision (ICD-11), officially
recognizing DRM as a pathological entity5.
Disease-related malnutrition in cardiac surgery
Patients undergoing cardiac surgery have a greater predisposition to DRM, as a consequence of
the pathophysiological response to the underlying disease and surgical trauma, characterized by
neurohormonal , metabolic, immunological, and inflammatory alterations that lead to the activation
of proteolytic pathways and muscle wasting, anorexia, early satiety, malabsorption, and reduced
functional capacity6,7.
Malnutrition in this patient group is associated with a higher risk of cardiac
and gastrointestinal complications, prolonged hospital stays, greater need for antibiotic therapy
and vasopressor support, increased healthcare costs, and a lower overall survival rate8-11. Although
recognized as a high-risk nutritional and clinical group, these patients have the highest rates of
iatrogenic malnutrition12,13. This is possibly due to the
lack of validated criteria for their nutritional
diagnosis14, following the precept
that what is not detected cannot be treated.
Global Leadership Initiative on Malnutrition
The Global Leadership Initiative on Malnutrition (GLIM) was launched in 2016 with the participation
of multiple scientific societies of clinical nutrition from Europe, Asia, North America and South
America. In 2019 the official document of the initiative was published, presenting the diagnostic
criteria for DRM15, which are
intended to be universally accepted and allow for the standardization
of malnutrition diagnosis. The GLIM criteria have been translated into Spanish and have face and
content validity as they come from expert judgment; however, the authors point out that their
criterion validity and reproducibility in different populations and clinical groups need to be evaluated
before their incorporation into medical practice16.
Gaps in literature
A systematic review identified more than 61
criterion validation studies of the GLIM criteria; however,
none included patients undergoing cardiac surgery17. To the best of our knowledge, only Liu et al.11 have evaluated the GLIM
criteria in this population, in an Asian cohort. Their study focused on the
predictive validation of the criteria, so gaps remain regarding concurrent criterion validity and interrater
reliability in this group of patients. Furthermore, the external applicability of Liu's findings to
Latin American populations is limited due to sociodemographic and biological differences among
patients. In Colombia, to our knowledge, no GLIM criterion validation studies have been conducted
in any clinical setting18,
reflecting the lack of local data to support its implementation.
Based on the scenario described, the objective of this research was to determine the
concurrent and
predictive criterion validity, and the inter-rater reliability of the GLIM criteria in Colombian patients
undergoing cardiac surgery.
Materials and Methods
Study population and design
This was a criterion validation study in a cohort of 51 adult patients (≥18 years) hospitalized with
an indication for cardiac surgery, who agreed to participate voluntarily in the study, at a highcomplexity
health center in the city of Medellín-Colombia. Patients with the following were excluded:
cancer, critical illness, neurocognitive disorders or altered state of consciousness that prevented the
administration of the tests (e.g. major neurocognitive disorder, delirium), neuromuscular diseases
(e.g. myasthenia gravis), and previous major surgery during the same hospitalization.
This research used census sampling: all participants who met the selection criteria during
the study
period (April–August 2024) were included. There is no unified criterion in the literature regarding
the sample size required for evaluating the psychometric properties of health measurement scales.
Different authors and scientific societies endorse the rule of thumb or the subject-item ratio, which
suggests including at least 10 participants for each variable assessed on the scale19,22. In the case of
the GLIM criteria, this corresponds to a minimum sample size of 50 participants.
Ethical statement
This study was conducted in accordance with the ethical principles for medical research involving
human participants established by the Declaration of Helsinki (World Medical Association) and
Colombian Resolution 008430 of 199323. Based on the national resolution, it was classified as
a
minimal-risk study. The procedures, techniques, and instruments were approved by the Clinic's Ethics
Committee (Minutes No. 216, January 25, 2024). Written informed consent was obtained from all
participants.
Nutritional diagnosis based on GLIM criteria
The diagnosis of malnutrition by GLIM requires the combination of at least one phenotypic criterion
and one etiological criterion. Phenotypic criteria include involuntary weight loss, low body mass index
(BMI), and reduced muscle mass. Etiological criteria include: involuntary decrease in food intake (<50% of
the recommended intake for more than one week or any reduction in intake for more than two weeks),
presence of digestive disease or symptoms that negatively affect nutrient absorption, and
disease-related inflammation (acute or chronic illness, infection, or injury that is usually associated
with inflammatory activity). Subsequently, the degree of malnutrition (moderate or severe) is classified
based on defined cut-off points for the phenotypic criteria Table 115.
Table 1. Cut-off points for determining the severity of malnutrition
X
Table 1. Cut-off points for determining the severity of malnutrition
Degree of
malnutrition
|
Unintentional weight
loss
|
Body mass index
|
Reduction in muscle mass
(calf circumference) *
|
|
Moderate malnutrition
|
>5-10% in the last 6 months or
>10-20% in more than 6 months
|
<20 kg/m2 si <70 years
<22 kg/m2 si ≥70 years |
<34 cm male
<33 cm female |
|
Severe malnutrition |
>10% in the last 6 months or
o
>20% in more than 6 months
|
<18.5 kg/m2 si <70 years
<20 kg/m2 si ≥70years |
<32 cm male
<31 cm female |
Note: Adapted from Cederholm et al.15
and Gonzalez al.24
*In this study, calf circumference was used as an
indicator of muscle
mass, considering its availability, portability, low cost,
simplicity (minimal training) and quick application; using
cut-off points
validated against the Gold Standard of body composition ( dual
energy X-ray absorptiometry)24
Evaluation of GLIM criteria
1. BMI:
The weight and height of the participants were measured using a digital scale with a
built-in stadiometer (SECA 777), with sensitivities of 0.1 kg and 0.1 cm respectively. BMI was
established using the formula: weight (kg) / height (m)
2.
2. Weight loss: Usual weight was obtained from previous medical records provided the data
was no
older than 12 months. If this was unavailable, the patient was asked directly. The percentage of
weight loss was calculated using the formula: (usual weight – current weight) / usual weight *100.
3. Muscle mass: Was estimated by measuring calf circumference (CC) with a Lufkin W606PM
anthropometric tape (sensitivity 0.1 cm). The value obtained was classified according to the cutoff
points suggested by González24 Table 1. In cases of excess weight, the CC value was adjusted
by subtracting the estimated subcutaneous adipose tissue, as follows: -3 cm in overweight, -7
cm in grade I and II obesity and -12 cm in grade III-V obesity24. In addition, in cases of lower
limb edema, 2 cm were subtracted for men and 1.6 cm for women25. For all anthropometric
measurements, institutional protocols were followed.
Additionally, muscle strength was assessed using a CAMRY EH101 handheld digital
dynamometer (sensitivity 0.1 kg), which has demonstrated excellent validity and reliability
compared to the JAMAR dynamometer26, representing a cost-effective alternative. Following
the diagnostic algorithm and cut-off points proposed at the second meeting of the European
Working Group on Sarcopenia in Older Adults (EWGSOP2), patients were classified as having
probable sarcopenia (dynapenia) when their strength was below 27 kg in men and 16 kg in
women27. Patients with low
strength and muscle mass were classified as having confirmed
sarcopenia27. Physical performance
was not assessed.
4. Intake: The patient was directly asked about their food intake over the past two weeks.
If there
had been an involuntary reduction, the percentage decrease was determined by using their
usual diet as a reference (plate method).
5. Digestive disease or symptoms: The following diagnoses or background information
recorded
in the admission medical history were considered: bariatric surgery, short bowel syndrome,
pancreatic insufficiency, gastroparesis, high output ostomy (>500 ml/24h), dysphagia and
esophageal stenosis, or the presence of diarrheal disease, steatorrhea and vomiting in the last
week15.
6. Disease-related inflammation: Was assumed to be part of decompensated cardiovascular
disease and, when available, was confirmed with a C-reactive protein ≥3 mg/dL28.
Nutritional diagnosis based on Subjective Global Assessment
Subjective Global Assessment (SGA) is a universally accepted tool for the assessment of nutritional
status, with application in various patient groups and care settings, and has therefore been
traditionally used as a reference standard for the validation of new diagnostic methods29. The SGA is
based on the evaluation of the patient's medical history (involuntary changes in weight and dietary
intake, functional capacity, gastrointestinal symptoms with nutritional impact and metabolic stress
associated with the disease) and on the nutrition-focused physical examination, which aims to identify
subcutaneous fat loss, muscle wasting and the presence of edema or ascites29.
The creators of this tool suggest that, for diagnostic purposes, the assessment should focus on criteria
for weight loss, decreased intake, and physical examination findings such as loss of subcutaneous fat
and muscle wasting29,30. Based on the results, the
patient is classified into three categories: A (wellnourished),
B (moderately malnourished), and C (severely malnourished)29.
Although the classification of nutritional status is primarily qualitative, based on the
predominance
of signs and symptoms and the clinical judgment of the evaluator, the authors have suggested some
descriptions for each category30:
A. Well-nourished: patients with weight loss <5% in the last six months or ≥5% but with
recent weight gain (in the last two to four weeks) and improved appetite.
B. Moderately malnourished:
pacientes con pérdida de peso ≥5 - 10% en los últimos seis meses sin ganancia o
estabilización reciente, disminución de la ingesta alimentaria y pérdida leve del tejido subcutáneo.
C. Severely malnourished:
patients with weight loss >10% in the last six months, with severe loss
of subcutaneous tissue and muscle wasting, often with edema.
For the application of the questionnaire, the guidelines and directives established
by the authors
were followed30.
Inter-rater reliability
Inter-rater reliability assesses the agreement between at least two trained evaluators, evaluating
the
same patients, using the same instrument, and on the same occasion31. For this purpose, all patients
received a direct preoperative nutritional assessment, based on the GLIM criteria, by two clinical
nutrition professionals, who performed the assessments independently and recorded the results in
isolated databases to ensure blinding. The assessments were carried out on the same day.
Concurrent criterion validation
Concurrent criterion validity refers to the degree to which the results of a scale are valid when
compared
with the results of other certified instruments known as gold standards31.
The GLIM validation guide16 established the SGA as a reference standard, so
a third, blinded, and trained professional performed
a new preoperative nutritional assessment according to the SGA, with a difference of 24 hours from
the GLIM assessments.
Predictive validation
The predictive criterion validity determines the agreement between the scale result (malnutrition)
with an event related to the phenomenon that may occur in the future (clinical outcome)16. According to the
validation guide, to establish predictive validity in the hospital setting, outcomes
such as hospital mortality, major complications, readmission and length of stay, which are expected
to be associated with malnutrition, should be considered16. After surgery, patients were monitored
through their medical records during their hospital stay and on day 30 post-discharge to determine
the occurrence of outcomes. Follow-up was conducted in real time while the patient remained in the
institution; therefore, missing data from the medical record were obtained by consulting directly
with
the attending physician, without requiring data entry. Furthermore, it was ensured that these were
incidental outcomes and not prevalent ones.
The outcomes were segmented into one primary outcome and nine secondary outcomes. The
secondary outcomes included the incidence of hospital mortality, sepsis and shock (from any cause)
after surgery, surgical reintervention, length of hospital stay, length of stay in the intensive
care unit
(ICU), and operative times (surgical, clamping, and perfusion). Outcome confirmation was based on
medical records.
For predictive validation, the primary outcome was hospital readmission within 30 days. This had
to be readmission to the same health center and for causes associated with the surgery, according
to the criteria of the emergency physician (e.g., surgical site infection, bleeding, wound
dehiscence,
pneumothorax, dyspnea, pleural effusion, hypotension, and uncontrolled pain).
Covariates
The following variables were obtained from clinical records and pre-anesthetic assessment: age,
sex, smoking habit, alcohol consumption, left ventricular ejection fraction (%LVEF), functional
classification New York Health Association (NYHA), cardiac surgery mortality score Society of
Thoracic Surgeons (STS), nutritional support, number of chronic diseases, hemoglobin, white blood
cell count,
neutrophil-to-lymphocyte ratio, and creatinine. For laboratory results, the time window was limited
to
7 days prior to the nutritional assessment. When multiple results were available, the most recent
was
included. Patients were also classified according to the type of surgery and the valves operated on.
The information was recorded in a database designed in Microsoft Excel, which included validations
and restrictions to minimize data entry errors. The tool was evaluated through a pilot test with 10
participants from the study population. In case of doubts or inconsistencies, the research team
verified
the information directly with the treating professional. This was possible thanks to the prospective
design of the research.
Statistical analysis
Analyses were performed using the Jamovi statistical platform, version 2.3.21 (The Jamovi Project
2023), and the R statistical software, version 4.4.0 (R Core Team 2024). Quantitative variables are
summarized using mean and standard deviation or median and interquartile range. Normality was
assessed using the Shapiro-Wilk test. Categorical variables are summarized using absolute and
relative
frequencies. To compare baseline characteristics according to nutritional status, the student’s
t-test or
Mann-Whitney U test was used for quantitative variables, and the chi-square test of independence or
Fisher's exact test was used for qualitative variables.
Inter-rater agreement was determined using Cohen's kappa index weighted by squared
weights
for ordinal scales. Classification was based on the Landis and Koch criteria32. The cutoff point for
determining inter-rater reliability was >0.816. For concurrent criterion validity, the simple
kappa
index was used, and diagnostic performance measures (sensitivity, specificity, predictive values,
and
diagnostic odds ratio). Validation was achieved if both sensitivity and specificity were greater
than
80%16.
For predictive criterion validation, a robust variance generalized linear regression
model (Poisson
family) was performed to obtain simple and adjusted relative risks (RR). Predictive validity was
concluded if the effect size was ≥ 2.016. The assumptions of this model were tested, and
the goodness
of fit was assessed using metrics such as deviance and pseudo-R². A multiple linear regression model
was also performed to establish the association between length of hospital stay (dependent) and
muscle mass (independent). The model assumptions were corroborated, and the goodness of fit was
assessed using R² and the F-test for overall significance. The adjustment variables for both models
were selected based on clinical criteria. All collected data are freely available for consultation
on Mendeley Data33.
Results
Characterization of the study population
The baseline characteristics of the participants are described in Table
2. According to nutritional
status, there was a statistical difference in the proportion of confirmed sarcopenia, being
significantly
(p=0.001) higher in people with malnutrition (46.43%) compared to those with adequate nutritional
status (4.35%).
Table 2. Sociodemographic and Clinical Characterization According to Nutritional Status
X
Table 2. Sociodemographic and Clinical Characterization According to
Nutritional Status
| Basic features
|
General (n=51)
% (n)
|
Well nourished
(n=23)
% (n)
|
Malnutrition
(n=28)
% (n)
|
p-value*
|
|
Sex, male
|
62.75 (32)
|
65.22 (15)
|
60.71 (17)
|
0.74 ‡
|
|
Age (years)ª
|
64.14 ± 11.00
|
62.87 ± 11.75
|
65.18 ± 10.45
|
0.46 †
|
|
LVEFb
|
55.00 [50.00;60.00]
|
55.00 [50.00; 60.00]
|
55.00 [50.00; 60.00]
|
0.66
|
|
STSb
|
1.32 [0.80; 2.49]
|
1.30 [0.76; 1.85]
|
1.45 [0.93; 2.71]
|
0.34
|
|
Nutritional support
|
19.61 (10)
|
13.04 (3)
|
25.00 (7)
|
0.48
|
|
Chronic diseasesb
|
3.00 [2.00; 4.00]
|
3.00 [2.00; 4.00]
|
3.00 [2.00; 5.00]
|
0.93
|
|
Hemoglobin (g/ dL)a
|
14.36 ± 1.72
|
14.70 ± 1.68
|
14.09 ± 1.73
|
0.22 †
|
|
Leukocytes (103 uL)a
|
8.67 ± 2.54
|
8.19 ± 2.26
|
9.07 ± 2.73
|
0.24 †
|
|
Neutrophil/ lymphocyte ratiob
|
2.56 [1.78; 3.56]
|
2.73 [1.90; 3.36]
|
2.55 [1.77; 3.58]
|
0.90
|
|
Creatinine (g/dL)b
|
0.90 [0.77; 1.18]
|
0.92 [0.78; 1.10]
|
0.90 [0.75; 1.21]
|
0.93
|
|
Smoker asset
|
13.73 (7)
|
8.70 (2)
|
17.86 (5)
|
0.46
|
|
Alcohol consumption
|
11.76 (6)
|
17.39 (4)
|
7.14 (2)
|
0.39
|
|
Grip strength (kg)b
|
27.45 [20.05;33.35]
|
27.15 [21.20; 41.15]
|
23.00 [19.20; 27.90]
|
0.06
|
|
Probable sarcopenia
|
43.14 (22)
|
34.78 (8)
|
50.00 (14)
|
0.39 ‡
|
|
Confirmed sarcopenia
|
27.45 (14)
|
4.35 (1)
|
46.43 (13)
|
0.001
|
|
Type of surgery
|
|
|
|
0.14
|
|
Revascularization myocardium
|
65.96 (31)
|
54.55 (12)
|
76.00 (19)
|
|
|
Valvular
|
19.15 (9)
|
31.82 (7)
|
8.00 (2)
|
|
|
Combined
|
14.89 (7)
|
13.64 (3)
|
16.00 (4)
|
|
a:Mean ± standard deviation; b:Median [interquartile range]; *Mann-Whitney U test for quantitative variables and Fisher's
exact test for categorical variables, unless otherwise indicated. † Student's t-test for independent samples; ‡ Chi-square test
of independence (Sex, probable sarcopenia) or Fisher's exact test (for all others). LVEF: Left ventricular ejection fraction; STS:
Society of Thoracic Surgeons operative mortality score.
Preoperative prevalence of malnutrition according to GLIM criteria
More than half of the participants presented with some degree of malnutrition (54.90%). Reduced
muscle mass was the most frequent phenotypic criterion; 45.10% of patients exhibited moderate or
severe muscle depletion. The predominant etiological criterion was reduced food intake (37.25%).
Inflammation was a constant finding.
Inter-rater reliability
An almost perfect agreement was found in the nutritional diagnosis by GLIM between the two
professionals (Kappa 0.94, 95% CI 0.88-0.99, p <0.001) verifying the inter-rater reliability of
these criteria.
Concurrent validity
Nutritional diagnosis using GLIM showed substantial agreement with diagnosis using SGA (Kappa
0.64,
95% CI 0.44–0.85, p <0.001). GLIM identified 88.00% of patients with malnutrition (Sensitivity
88.00, 95% CI 68.78–97.45) and 76.92% of well-nourished patients (Specificity 76.92, 95% CI
56.35–91.03). Diagnostic accuracy was 82.35%, and the positive and negative predictive
values were 78.57% and 86.96%, respectively. The probability of correctly diagnosing
nutritional status with GLIM is 24.44 times the probability of making a mistake (ORd 24.44,
95% CI 5.39–110.92).
Association between nutritional status and clinical outcomes
Of the 51 patients evaluated, 4 declined surgical intervention (n=47): 3 with malnutrition
and 1 with adequate
nutritional status. No statistically significant differences were observed in the incidence
of secondary outcomes according to overall nutritional status Table
3. However, an inverse linear association was found
between calf circumference and length of hospital stay, which remained after adjusting the
model (β -0.47,
95% CI -0.89 to -0.05, p 0.03) Figure 1. It was also reported that for
each concomitant chronic disease, the
length of hospital stays increased by 1.3 days (β 1.32, 95% CI 0.19 to 2.45, p 0.02) Figure 1
Table 3. Postoperative outcomes according to nutritional status
Ver Más
X
Table 3. Postoperative outcomes according to nutritional status
|
Clinical outcomes
|
General (n=47)
% (n)
|
Well nourished (n=22)
% (n)
|
Malnutrition
(n=25)
% (n)
|
p-value*
|
|
Days of stay in ICUb
|
3.00 [2.00; 4.00]
|
3.0 [1.25; 4.00]
|
3.00 [2.00; 5.00]
|
0.61
|
|
Days of hospital stayb
|
6.00 [5.00; 8.50]
|
6.00 [5.00; 7.00]
|
7.00 [5.00; 10.00]
|
0.11
|
|
Hospital mortality
|
6.38 (3)
|
9.09 (2)
|
4.00 (1)
|
0.59
|
|
Shock for any reason
|
21.28 (10)
|
31.82 (7)
|
12.00 (3)
|
0.15
|
|
Surgical reintervention
|
6.38 (3)
|
9.09 (2)
|
4.00 (1)
|
0.33
|
|
Sepsis
|
8.51 (4)
|
0.00 (0)
|
16.00 (4)
|
0.11
|
|
Surgical time (min)b
|
300.00 [300.00;330.00]
|
300.00 [247.50; 330.00]
|
300.00 [300.00; 300.00]
|
0.33
|
|
Infusion time (min)b
|
124.00 [93.00; 139.00]
|
130.50 [72.00; 144.25]
|
123.00[101.00; 139]
|
1.00
|
|
Clamp time (min)b
|
103.00 [70.00; 123.00]
|
109.00 [58.75; 128.25]
|
97.00 [84.00; 120.00]
|
0.84
|
b
Median [interquartile range], min: minutes. *Mann-Whitney U
test for quantitative variables and Fisher's exact test for
qualitative variables.
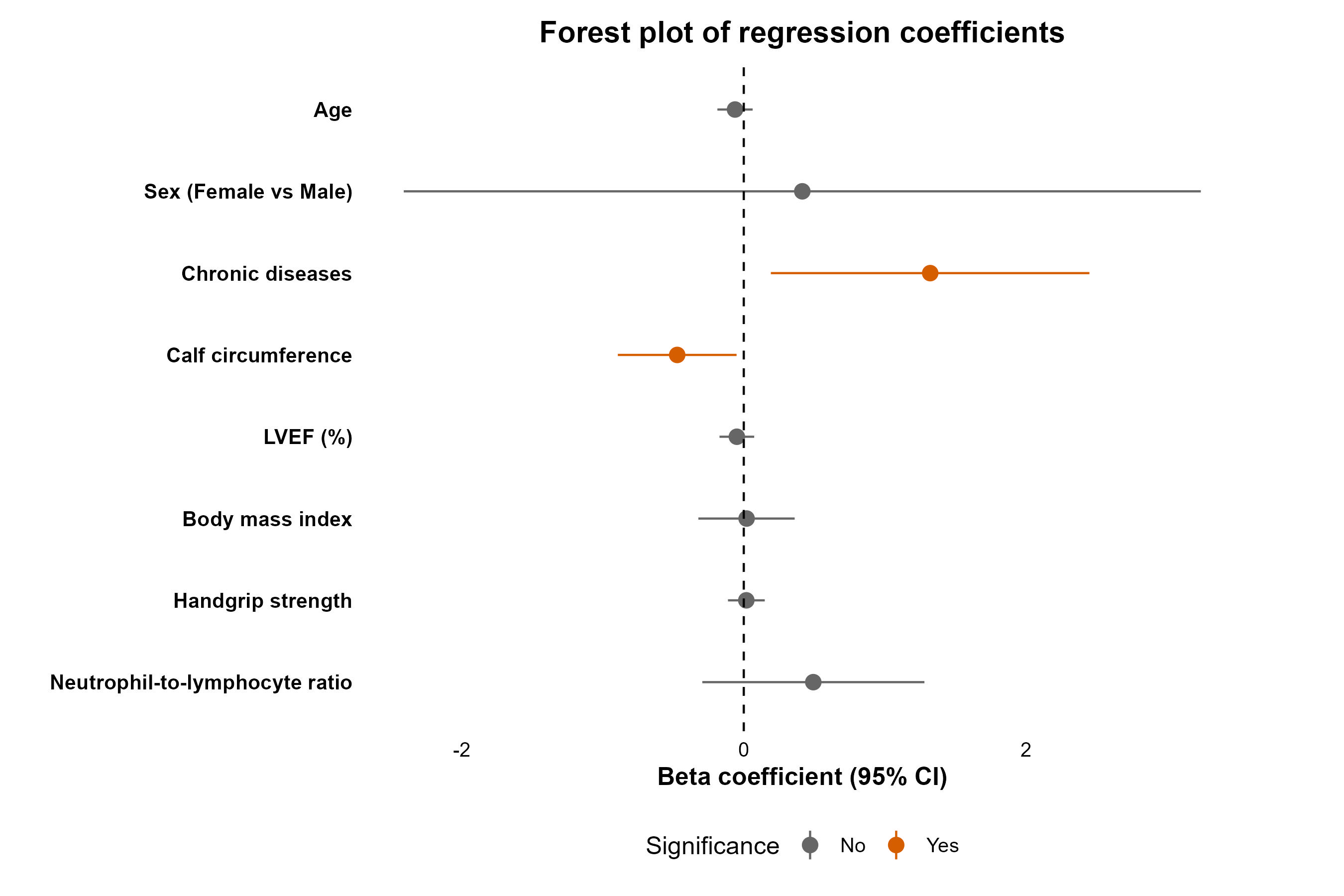
Figure 1. Association between calf circumference and days of
hospital stay
Each circle in the graph represents the regression coefficient (β), which indicates the
estimated change
in length of hospital stay for each unit change in each independent variable. Positive
coefficients
reflect an increase in length of stay, while negative coefficients indicate a decrease.
The horizontal
lines show the 95% confidence intervals. The vertical line plotted at zero represents
the point of nonsignificance;
if an interval includes zero, it suggests no statistical association between the
variables.
Fitted model: normality of residuals (Shapiro-Wilk p = 0.52); independence of errors (DW
statistic 2.25,
p = 0.42); homoscedasticity (Breusch - Pagan p = 0.06); all variance inflation factors
were less than two.
-R2 0.440. RMSE 2.95. Global Model Test p = 0.01. Adjusted for age, sex,
number of chronic diseases,
left ventricular ejection fraction (%), body mass index, grip strength, and
neutrophil-lymphocyte
index.
Predictive criterion validity
GLIM malnutrition acted as a risk factor for hospital readmission at 30 days.
Patients with
malnutrition had a 1.59 times greater risk of readmission due to post-surgical
complications than
patients with adequate nutritional status, confirming the predictive criterion
validity (RRa 2.59, 95%
CI 1.09 – 7.02, p 0.04)Table 4.
Table 4.Association between nutritional status and hospital readmission
at 30 days
X
Table 4. Association between nutritional status and hospital
readmission at
30 days
|
Variable
|
RR crude
CI 95%
|
RR djusted
CI 95%
|
p-value
|
|
Nutritional status
|
|
|
|
|
Well nourished
|
1
|
1
|
|
|
Malnutrition
|
2.45 (1.15 - 5.77)
|
2.59 (1.09 - 7.02)
|
0.04
|
|
Age
|
0.97 (0.95 - 1.01)
|
0.97 (0.93 - 1.01)
|
0.16
|
|
Sex
|
|
|
|
|
Femele
|
1
|
1
|
|
|
Male
|
1.19 (0.57 - 2.41)
|
1.19 (0.42 - 3.19)
|
0.73
|
|
%LVEF
|
0.99 (0.95 - 1.04)
|
0.99 (0.95 - 1.04)
|
0.71
|
|
Chronic diseases
|
1.05 (0.82 - 1.34)
|
1.16 (0.86 - 1.54)
|
0.32
|
|
Grip strength
|
0.99 (0.96 - 1.03)
|
1.01 (0.95 - 1.06)
|
0.76
|
RR: Relative
Risks - Adjusted for age, sex, number of chronic diseases, preoperative
left ventricular ejection fraction (%) and grip strength. All variance
inflation factors were less than 2.
Pseudo-R2 0.169 Deviance 27.
LVEF: Left ventricular ejection
fraction. Todos los factores de inflación de la varianza fueron menores
a 2.
Pseudo-R2
0.169
Devianza 27. FEVI: Fracción de eyección ventrículo
izquierdo.
Discussion
This study demonstrated the inter-rater reliability and
predictive validity
of the GLIM
operational
criteria in a group of Colombian patients undergoing cardiac
surgery.
Although the specificity
threshold for concurrent criterion validity was not reached, the
overall
results suggest
acceptable
diagnostic performance for malnutrition.
Few studies have explored the validity of GLIM in
the context
of cardiac surgery.
A retrospective
analysis conducted by Thomas et al.34 in 224
patients from a
vascular surgery
unit in Australia, found
moderate diagnostic agreement (Kappa 0.42) between GLIM and
patient-generated subjective global
assessment (PG-SGA), with a sensitivity of 73.7% (95% CI
52.8-94.8) and a
specificity of 80.6%
(95% CI
75.2-86.0%). In 119 Spanish adults hospitalized for acute
medical
conditions, including a
subgroup
of patients with cardiovascular disease (9.2%), substantial
agreement (Kappa
0.64, 95% CI
0.50–0.79)
was observed between GLIM and SGA, with a reported sensitivity
of 78% (95%
CI 64.0–88.5) and
specificity of 86.2% (95% CI 75.3–93.5)35. The
studies described
present findings
moderately like
those of the present investigation. None managed to demonstrate
concurrent
criterion validity by
not reaching the sensitivity and specificity thresholds (>80%)
(15) .
However, a prospective
cohort
study conducted in five high-complexity hospitals in Brazil
(n=601),
demonstrated the concurrent
validity of the GLIM criteria versus the SGA, in hospitalized
adults with
chronic conditions
(12.9%
for cardiovascular disease) and undergoing surgical
interventions, with a
sensitivity of 86.6%
and a
specificity of 81.6% 36.
The proportion of malnutrition determined by
GLIM differs
from that obtained by
SGA or PG-SGA34-36.
This is primarily due to the methods used to measure muscle
mass, a
predominant criterion in the
diagnosis of malnutrition37 qthat is
closely
related to health
outcomes38. SGA is
based on the detection
of qualitative signs of muscle depletion through physical
examination, which
can underestimate
low muscle mass, especially in patients with abundant
subcutaneous adipose
tissue 39. In
contrast,
GLIM suggests the use of body composition technologies such as
bioelectrical
impedance, computed
tomography, ultrasound, and dual-energy X-ray absorptiometry
(DXA), or,
failing that,
anthropometric
measurements such as calf circumference, which has been
validated against
these methods and for
which cut-off points and adjustments have been determined to
improve its
validity24,39,40
.
Preoperative muscle mass is a predictor of
hospital stay in
cardiac surgery
patients. Zuckerman et al.41 reported in
a cohort of
older adults, that
for every centimeter increase in psoas muscle area,
postoperative hospital stay decreased by 2.35 days (β –2.35, 95%
CI –4.48 to
–0.22). In patients
undergoing transcatheter aortic valve replacement (TAVR), an
increase in
skeletal muscle index
was found to be associated with a one-day reduction in hospital
stay (p
0.03)42 y Shibasaki
et
al.43 and
Shibasaki et
al.43 demonstrated in cardiac surgery patients that sarcopenia
(decreased
muscle mass and
function)
was the factor most strongly associated with prolonged stay (>20
days) (OR
2.507, 95% CI 1.138 –
5.521, p <0.05). Our study also revealed an inverse association
between muscle mass, measured by calf circumference, and
postoperative stay. These findings are consistent with those
reported by Tarnowski44
in hospitalized patients, who highlighted
an increased probability of prolonged
hospitalization (>16 days) in patients with decreased calf
circumference
(OR 1.59, 95% CI
1.07 – 2.36,
p 0.023).
Patients undergoing cardiac surgery are prone to
muscle
wasting during
hospitalization due to the
inflammatory response to surgical stress and factors such as
immobility or
deterioration of
functional
status, the need for mechanical ventilation, and malnutrition,
exacerbating
deficits present at
admission14,45. In the
first
postoperative week, a 16% reduction in the transverse area of
the rectus
femoris and a 24% reduction in the pennation angle have been
described45. Muscle
waste in
the first
week after cardiac surgery prolongs the ICU stay and the need
for mechanical
ventilation46.
Muscle mass is also part of the operational definition of
sarcopenia27,
47, understood
as a
progressive
and generalized musculoskeletal disorder, associated with adverse health
outcomes27.
Malnutrition
has been recognized as one of the main predictors of sarcopenia (HR 3.23,
95% CI 1.73 – 6.05)
and
severe sarcopenia (HR 2.87, 95% CI 1.25 – 6.56)48
and both conditions can coexist in patients
with
cardiovascular disease, increasing the risk of death in the medium and long
term49,50. Therefore,
GLIM
considers the association between nutritional status and syndromes such as
sarcopenia and
frailty,
theoretically related to malnutrition, as an indirect form of validation,
which it defines as
convergent
construct validity, determined through hypothesis testing (X2 p <0.05 if n: <200 or p<0.01
if n: ≥200) (X2 p <0,05 si n: <200 o p<0,01 si n: ≥200)16. This
study
provides theoretical
evidence that supports the construct validity of GLIM in the context
of cardiac surgery, by reaffirming the association between
malnutrition and sarcopenia
(p <0.001, difference of proportions 0.421, 95% CI 0.21 – 0.62).
Regarding the predictive criterion validity,
hospital
readmission within 30 days was selected as the
primary outcome16,
considering the low
incidence of postoperative outcomes during the hospital
stay, which is related to short hospital observation times
after the
intervention (median 6 days).
Cardiac surgery patients tend to have short stays in both
the ICU and the
hospital, which can make it
difficult to identify intermediate and late
complications46,
51.
To our knowledge, only one study has explored the predictive
validity of GLIM in
cardiac surgery. Liu et al.11
conducted an observational
study in 603 adult patients from the cardiothoracic surgery
department of Tenth People's Hospital in Shanghai,
undergoing myocardial
revascularization or valve
surgery, showing that malnutrition was associated with
postoperative
complications (Clavien -Dindo
≥2) (OR 1.66, 95% CI 1.063–2.594, p 0.026) and lower overall
survival at
three-year follow-up (HR 2.339,95% CI 1.504–3.637, p
<0.001). These findings were confirmed in a post hoc analysis in older
adults (≥65 years) (n=401), although in this group the threshold (HR,
RR, OR>2) for the
predictive
criterion
was not reached (HR 1.862, 95% CI 1.171–2.962, p
0.009)52.
Liu's study did not describe hospital
readmission; however, in
internal medicine patients, GLIM
malnutrition has been shown to increase the 30-day
readmission risk by 66% (RR
1.66, 95% CI 1.06–
2.62, p 0.026)53.
Furthermore, in a cohort
of cancer patients (n = 2801), in which the validity of
three
diagnostic malnutrition scales was compared, GLIM
demonstrated the best
predictive capacity for
unplanned admission and 30-day readmission (OR 1.78, 95% CI
1.34–2.35, p < 0.001)54. The
literature
highlights an increased risk of readmission in
malnourished individuals,
which we have reported in
our study.
No studies have been identified that
evaluate the
inter-rater reliability of GLIM in cardiac surgery.
However, in patients with gastrointestinal cancer
(n=1115),Tan et al.55
reported substantial agreement
between independent evaluators when all diagnostic
categories were included
(Kappa 0.78, 95%
CI 0.74–0.82). Similarly, in patients with head and neck
cancer (n=188),
almost perfect agreement
(Kappa 0.985) was observed between trained
dietitians56.
Together
with our
results, these findings
support the reproducibility and clinical applicability
of GLIM.
Given this scenario, the need for timely
detection of
malnutrition in cardiac surgical patients through
methodologies such as GLIM, and the implementation of
nutritional
prehabilitation programs is
highlighted, with the objectives of mitigating the
nutritional impact of the
disease and the surgical
procedure, and optimizing health outcomes, as suggested by
the ERAS
guidelines57.
An example of
this is the preoperative administration of oral nutritional
supplements high in
protein or enriched
with immunonutrients, which appear to reduce weight loss,
the rate of infectious
and non-infectious
complications and hospital stay58,59.
Strengths and limitations
This study has some limitations. First, the sample size was
small, which may
have affected the accuracy
of the results and the statistical power needed to identify
other associations.
Second, the diagnosis
of outcomes was based on the treating physician's judgment.
Adherence to
standardized diagnostic
criteria or clinical practice guidelines was not assessed.
Third, this was a
single-center study of patients
with severe coronary or valvular heart disease, most of whom
were admitted in
the context of an
acute coronary syndrome. This limits the generalizability of
the results and
reduces the representation
of patients with milder forms of the disease or those
scheduled for elective
surgery, in whom the
prevalence of malnutrition may be lower. Fourth, hospital
readmission was only
recorded for the
institution where the surgery was performed. Some patients
may have experienced
postoperative
complications and sought care at other healthcare facilities
(loss to
follow-up). Finally, the nutritional
assessment included criteria such as weight loss and reduced
food intake, both
of which are subject to
potential bias. Usual weight may be inaccurate due to
imprecise patient recall
or unreliable previous
records, and the reduction in intake was based on
self-report, which introduces
subjectivity.
Among the strengths of this study, it is
noteworthy that, to the
authors' knowledge, it is the first
to jointly and prospectively evaluate the concurrent and
predictive criterion
validity, as well as the
inter-rater reliability, of the GLIM criteria in cardiac
surgery patients.
Furthermore, it is the first GLIM
criterion validation study in Colombian patients.
Nutritional status assessment
was performed by
trained professionals (primary source) using validated
techniques and cut-off
points. The prospective
nature of this research ensured the temporality of the
events (malnutrition –
outcome).
Recommendations for future
research
Long-term longitudinal cohort studies with larger,
multicenter samples are
suggested to improve
the generalizability of the findings. Furthermore,
incorporating body
composition technologies such
as DXA is recommended to achieve a more objective
nutritional and functional
assessment, which
would also allow for the exploration of other phenotypes
such as sarcopenic
obesity. Finally, local,
controlled, randomized clinical trials are needed to
evaluate whether early
nutritional interventions
optimize clinical and economic outcomes in this patient
group and to determine
the type and
duration of such interventions.
Conclusion
The GLIM criteria are reliable for diagnosing
malnutrition and
have predictive validity for relevant
clinical outcomes in patients undergoing cardiac surgery,
supporting their
utility and applicability
in clinical practice. Although the established specificity
threshold for
concurrent validation was not
reached, the overall diagnostic capacity of these criteria
was satisfactory.
Consequently, GLIM can be
considered a tool for nutritional diagnosis in this
population, as well as for
the timely identification
of patients eligible for nutritional prehabilitation
programs, with the aim of
optimizing their clinical
outcomes.
Conflicts of interest: The authors have no
conflicts of interest
to declare that are relevant to the
content of this article.
Funding: This research did not receive any
specific grants from
funding agencies in the public,
commercial, or non-profit sectors.
Acknowledgments: We express our sincere
gratitude to the
patients who participated in this study.
Their contribution was fundamental to the success of this work.
Author Contributions: Mateo Londoño-Pereira:
Conceptualization, formal analysis, investigation,
methodology, visualization, writing—original draft preparation,
writing—review and editing. Maite
Catalina Agudelo-Cifuentes: Methodology, supervision, visualization,
writing—review and editing.
Nora Elena Múnera: Investigation, methodology, writing—review and editing.
Sara Catalina Paredes:
Investigation, methodology, writing—review and editing. Maritza Londoño
Ramirez: Investigation,
methodology, writing—review and editing. Mónica Yepes Molina: Investigation,
methodology,
writing—review and editing.
References
-
Cederholm T, Bosaeus I. Malnutrition
in Adults. N
Engl J
Med. 2024;391(2).
https://doi.org/10.1056/nejmra2212159
-
Schuetz P, Seres D, Lobo DN, Gomes F,
Kaegi-Braun N, Stanga
Z. Management of diseaserelated
malnutrition for patients being treated in hospital. Lancet.
2021;398(10314):1927-
1938.
https://doi.org/10.1016/s0140-6736(21)01451-3
-
Jobim Milanez DS, Razzera EL, da Silveira
Knobloch I, Lima J,
Bernardes S, Silva FM.
A
scoping review on the GLIM criteria for malnutrition diagnosis:
Understanding how and
for
which purpose it has been applied in studies on hospital settings.
Clin Nutr.
2023;42(1):29–44.
https://doi.org/10.1016/j.clnu.2022.10.022
-
Correia MITD, Perman MI, Waitzberg
DL.
Hospital malnutrition in Latin America: A
systematic review. Clin Nutr. 2017;36(4):958-967.
https://doi.org/10.1016/j.clnu.2016.06.025
-
Uenishi M, Song P. New diagnostic
code “5B72
Undernutrition
in Adults” approved for
inclusion in the 11th Revision of the International Classification
of Diseases (ICD-11).
Drug
Discov Ther.
2025;19(6):437-439. https://doi.org/10.5582/ddt.2025.01118
-
Thanapholsart J, Khan E, Ismail TF, Lee
GA. The complex
pathophysiology of cardiac
cachexia: A review of current pathophysiology and implications for
clinical practice.
Am
J
Med Sci. 2023;365(1):9–18. https://doi.org/10.1016/j.amjms.2022.08.016
-
Savino Lloreda P, Posada Álvarez C, López
Daza
D.Nutrición
aplicada en patologías crónicas. 1ra ed. Colombia: Distribuna; 2020.
-
Mubashir T, Balogh J, Breland E, Rumpel D,
Waheed MA, Lai H, et
al. Risk Factors and
Outcomes of Protein-Calorie Malnutrition in Chronic Heart Failure
Patients Undergoing
Elective Cardiac Surgery. Cureus.
2022;14(10):e30378. https://doi.org/10.7759/cureus.30378
-
Unosawa S, Taoka M, Osaka S, Yuji D,
Kitazumi Y, Suzuki K, et
al.
Is malnutrition associated
with postoperative complications after cardiac surgery?
J Card Surg. 2019;34(10):908-912.
https://doi.org/10.1111/jocs.14155
-
Chermesh I, Hajos J, Mashiach T, Bozhko M,
Shani L, Nir RR, et
al. Segunda
Malnutrition in cardiac
surgery: food for thought. European Journal Preventive
Cardiology.
2014;21(4):475-483. https://doi.org/10.1177/2047487312452969
-
Liu Z, Shen Z, Zang W, Zhou J, Yu Z, Zhang
P, et al.
Development and Validation of Global
Leadership Initiative on Malnutrition for Prognostic Prediction in
Patients Who
Underwent
Cardiac Surgery.
Nutrients.
2022;14(12):2409. https://doi.org/10.3390/nu14122409
-
Drover JW, Cahill NE, Kutsogiannis J,
Pagliarello G, Wischmeyer
P,
Wang M, et al. Nutrition Therapy for the Critically Ill
Surgical Patient:
We
Need To Do Better!
J Parenter Enter
Nutr. 2010;34(6):644-652. https://doi.org/10.1177/0148607110372391
-
Rahman A, Agarwala R, Martin C, Nagpal D,
Teitelbaum M, Heyland
DK.
Nutrition Therapy
in Critically Ill Patients Following Cardiac Surgery: Defining and
Improving Practice.
J Parenter
Enter Nutr. 2016;41(7):1188-1194. https://doi.org/10.1177/0148607116661839
-
Stoppe C, Goetzenich A, Whitman G, Ohkuma R,
Brown T,
Hatzakorzian
R, et al.
Role
of nutrition support in adult cardiac surgery: a consensus statement
from an
International
Multidisciplinary Expert Group on Nutrition in Cardiac Surgery.
Crit Care.
2017;21(1):131. https://doi.org/10.1186/s13054-017-1690-5
-
Cederholm T, Jensen GL, Correia MITD,
Gonzalez MC, Fukushima R,
Higashiguchi T,
et al. GLIM criteria for the diagnosis of malnutrition
– A consensus report
from the global
clinical nutrition community. J Cachexia Sarcopenia Muscle.
2019;10(1):207-217. https://doi.org/10.1002/jcsm.12383
-
Keller H, Van Der Schueren MAE, GLIM
Consortium, Jensen GL,
Barazzoni R, Compher
C, et al.
Global Leadership Initiative on Malnutrition (GLIM): Guidance on
Validation of the
Operational Criteria for the Diagnosis of Protein‐Energy
Malnutrition in Adults. J
Parenter
Enter Nutr.
2020;44(6):992-1003. https://doi.org/10.1002/jpen.1806
-
Correia MITD, Tappenden KA, Malone A, Prado
CM, Evans DC, Sauer
AC,
et al. Utilization
and validation of the Global Leadership Initiative on Malnutrition
(GLIM): A scoping
review.
Clin Nutr. 2022;41(3):687-697
https://doi.org/10.1016/j.clnu.2022.01.018
-
Pérez A, Díaz Muñoz GA, Maza Moscoso CP,
Castro Muñoz MG,
Canicoba
ME, Gonzalez
MC, et al. Modelo de proceso de cuidado nutricional:
consenso para
Latinoamérica.
Rev Nutr
Clínica Metab.2022;5(4). https://doi.org/10.35454/rncm.v5n4.433
-
Roco Videla Á, Hernández Orellana M, Silva
González O.
¿Cual es el tamaño muestral
adecuado para Validar un cuestionario? Nutr Hosp.
2021;38(4):877-878. https://doi.org/10.20960/nh.03633
-
Morgado FFR, Meireles JFF, Neves CM, Amaral
ACS, Ferreira
MEC. Scale development:
ten main limitations and recommendations to improve future research
practices.
Psicol
Reflex
Crit. 2017;30:3. https://doi.org/10.1186/s41155-016-0057-1
-
Anthoine E, Moret L, Regnault A, Sébille V,
Hardouin
JB. Sample size used to validate a scale:a review of
publications on
newly-developed patient reported outcomes measures.
Health Qual Life Outcomes.2014;12:2. https://doi.org/10.1186/s12955-014-0176-2
-
International Test Commission. The
ITC Guidelines for
Translating and Adapting Tests
(Second edition). [Internet] 2017 [cited 2025 May 14]. Available
from:
www.InTestCom.org
-
Ministerio de Salud de Colombia.
Resolución 8430 de 1993, por la cual se establecen
las normas científicas, técnicas y administrativas para la
investigación en salud.
Bogotá:
Ministerio de Salud; 1993. Consulta: mayo 15, 2025. Disponible en:
minsalud.gov.co/sites/rid/lists/bibliotecadigital/ride/de/dij/resolucion-8430-de-1993.pdf
-
Gonzalez MC, Mehrnezhad A, Razaviarab N,
Barbosa-Silva TG,
Heymsfield SB.
Calf
circumference: cutoff values from the NHANES 1999–2006.
Am J Clin Nutr.
2021;113(6):1679-
1687. https://doi.org/10.1093/ajcn/nqab029
-
Ishida Y, Maeda K, Nonogaki T, Shimizu A,
Yamanaka Y, Matsuyama
R,
et al. Impact of
edema on length of calf circumference in older adults.
Geriatr Gerontol Int.
2019;19(10):993-
998. https://doi.org/10.1111/ggi.13756
-
Huang L, Liu Y, Lin T, Hou L, Song Q, Ge N,
et al.
Reliability and validity of two hand
dynamometers when used by community-dwelling adults aged over 50
years.
BMC Geriatr.
2022;22:580.
https://doi.org/10.1186/s12877-022-03270-6
-
Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y,
Bruyère O,
Cederholm T,
et al.
Sarcopenia:
revised European consensus on definition and diagnosis.
Age Ageing. 2019;48(1):16-31. https://doi.org/10.1093/ageing/afz046
-
Jensen GL, Cederholm T, Ballesteros‐Pomar
MD, Blaauw R, Correia
MITD, Cuerda C, et
al.
Guidance for assessment of the inflammation etiologic criterion for
the GLIM diagnosis
of
malnutrition: A modified Delphi approach.
J Parenter Enter Nutr. 2024;48(2):145-154. https://doi.org/10.1002/jpen.2590
-
Barbosa-Silva MCG, Barros AJ.
Indications and limitations of the use of subjective global
assessment in clinical practice: an update. Curr Opin Clin Nutr
Metab Care.
2006;9(3):263-269. https://doi.org/10.1097/01.mco.0000222109.53665.ed
-
Detsky AS, Smalley PS, Chang J.
Is this patient malnourished.
JAMA. 1994;271(1):54-58. https://doi.org/10.1001/jama.271.1.54
-
Luján-Tangarife JA, Cardona-Arias JA.
Construcción y validación de escalas de medición
en salud: revisión de propiedades psicométricas.
Archivos de Medicina.
2015;11(3:1). https://dialnet.unirioja.es/servlet/articulo?codigo=5178935
-
Landis JR, Koch GG.
The measurement of observer agreement for categorical data.
Biometrics.
1977;33(1):159–74. https://pubmed.ncbi.nlm.nih.gov/843571/
-
Londoño-Pereira M.
Validación criterios GLIM Cirugía Cardíaca. Mendeley
Data, V1.
2025.
https://doi.org/10.17632/349y7xs5st.1
-
Thomas J, Delaney C, Miller M. The
ability of the
Global
Leadership Initiative on Malnutrition
(GLIM) to diagnose protein–energy malnutrition in patients requiring
vascular surgery: a
validation study. Br J Nutr. 2023;129(1):49-53. https://doi.org/10.1017/s0007114522000344
-
Fontane L, Reig MH, Garcia-Ribera S, Herranz
M, Miracle M,
Chillaron
JJ, et al. Validity
and Applicability of the Global Leadership Initiative on
Malnutrition (GLIM) Criteria in
Patients Hospitalized for Acute Medical Conditions. Nutrients.
2023;15(18):4012. https://doi.org/10.3390/nu15184012
-
Brito JE, Burgel CF, Lima J, Chites VS,
Saragiotto CB, Rabito
EI, et
al.
GLIM criteria for
malnutrition diagnosis of hospitalized patients presents
satisfactory criterion
validity:
A prospective cohort study. Clin Nutr.
2021;40(6):4366-4372. hhttps://doi.org/10.1016/j.clnu.2021.01.009
-
Boslooper-Meulenbelt K, Van Vliet IMY,
Gomes-Neto AW, De Jong
MFC,
Bakker SJL, Jager-
Wittenaar H, et al. Malnutrition according to GLIM
criteria in stable
renal
transplant recipients:
Reduced muscle mass as predominant phenotypic criterion. Clin
Nutr.
2021;40(5):3522-3530. https://doi.org/10.1016/j.clnu.2020.11.034
-
Orsso CE, Montes‐Ibarra M, Findlay M, Van
Der Meij BS, De Van
Der
Schueren MAE, Landi
F, et al.
Mapping ongoing nutrition intervention trials in muscle,
sarcopenia, and
cachexia:
a scoping review of future research.
J Cachexia Sarcopenia Muscle.
2022;13(3):1442-1459. https://doi.org/10.1002/jcsm.12954
-
Compher C, Cederholm T, Correia MITD,
Gonzalez MC, Higashiguch
T,
Shi HP, et al. Guidance for assessment of the muscle
mass phenotypic
criterion
for the Global Leadership
Initiative on Malnutrition diagnosis of malnutrition.
J Parenter Enter Nutr. 2022;46(6):1232-1242.
https://doi.org/10.1002/jpen.2366
-
Prado CM, Landi F, Chew STH, Atherton PJ,
Molinger J, Ruck T, et
al.
Advances in muscle
health and nutrition: A toolkit for healthcare professionals.
Clin Nutr.
2022;41(10):2244-2263. https://doi.org/10.1016/j.clnu.2022.07.041
-
Zuckerman J, Ades M, Mullie L, Trnkus A,
Morin JF, Langlois Y,
et
al.
Psoas Muscle
Area and Length of Stay in Older Adults Undergoing Cardiac
Operations.
Ann Thorac Surg.
2017;103(5):1498-1504. https://doi.org/10.1016/j.athoracsur.2016.09.005
-
Dahya V, Xiao J, Prado CM, Burroughs P,
McGee D, Silva AC, et
al.
Computed tomography–
derived skeletal muscle index: A novel predictor of frailty and
hospital length of stay
after
transcatheter aortic valve replacement.
Am Heart J.
2016;182:21-27 https://doi.org/10.1016/j.ahj.2016.08.016
-
Shibasaki I, Ouchi M, Fukuda T, Tsuchiya G,
Ogawa H, Takei Y, et
al.
Effect of sarcopenia on
hospital stay from post cardiac surgery to discharge. IJC Heart
Vasc.
2022;39:101003.
https://doi.org/10.1016/j.ijcha.2022.101003
-
Tarnowski M, Stein E, Marcadenti A, Fink J,
Rabito E, Silva FM.
Calf Circumference Is a Good
Predictor of Longer Hospital Stay and Nutritional Risk in Emergency
Patients: A
Prospective
Cohort Study.
J Am Coll Nutr.
2020;39(7):645-649. https://doi.org/10.1080/07315724.2020.1723452
-
Buitrago NDC, Gallego DT, Pérez MCF, Cardona
CAQ, Botero CC.
Assessment of quadriceps muscle mass by ultrasound in the
postoperative period
of
cardiac surgery.
The Ultrasound Journal. 2024;16:8. https://doi.org/10.1186/s13089-023-00348-z
-
Dimopoulos S, Raidou V, Elaiopoulos D,
Chatzivasiloglou F,
Markantonaki D,
Lyberopoulou E, et al. Sonographic muscle mass
assessment in patients after
cardiac
surgery. World Journal Cardiology.
2020;12(7):351-361.
https://doi.org/10.4330/wjc.v12.i7.351
-
Kirk B, Cawthon PM, Arai H, Ávila-Funes JA,
Barazzoni R, Bhasin
S,
et al. The Conceptual
Definition of Sarcopenia: Delphi Consensus from the Global
Leadership Initiative in
Sarcopenia
(GLIS). Age and Ageing.
2024;53(3):afae052. https://doi.org/10.1093/ageing/afae052
-
Beaudart C, Sanchez-Rodriguez D, Locquet M,
Reginster JY,
Lengelé L,
Bruyère O.
Malnutrition as a Strong Predictor of the Onset of
Sarcopenia.
Nutrients. 2019;11(12):2883.
https://doi.org/10.3390/nu11122883
-
Ikeda S, Kodama A, Kawai Y, Tsuruoka T,
Sugimoto M, Niimi K, et
al.
Preoperative
sarcopenia and malnutrition are correlated with poor long-term
survival after
endovascular
abdominal aortic aneurysm repair. Surgery Today.
2022;52:98-105.
https://doi.org/10.1007/s00595-021-02362-x
-
Ohori K, Yano T, Katano S, Nagaoka R,
Numazawa R, Yamano K, et
al.
Coexistence of sarcopenia and self‐reported weight loss is a
powerful predictor of
mortality
in older
patients with heart failure. Geriatr Gerontol Int.
2024;24(1):95-101.
https://doi.org/10.1111/ggi.14778
-
Lee JJR, Srinivasan R, Ong CS, Alejo D,
Schena S, Shpitser I, et
al.
Causal determinants
of postoperative length of stay in cardiac surgery using causal
graphical learning.
J Thorac
Cardiovasc Surg. 2023;166(5):e446-462. https://doi.org/10.1016/j.jtcvs.2022.08.012
-
Liu Z, Zang W, Zhang P, Shen Z.
Prognostic implications of Global Leadership Initiative on
Malnutrition–defined malnutrition in older patients who underwent
cardiac surgery in
China.
Surgery.
2023;173(2):472-478. https://doi.org/10.1016/j.surg.2022.11.008
-
Cruz PL, Soares BLDM, Da Silva JE, Lima E
Silva RRD.
Clinical and nutritional predictors of hospital readmission within
30 days. Eur J
Clin
Nutr.
022;76:244-250. https://doi.org/10.1038/s41430-021-00937-y
-
Poulter S, Steer B, Baguley B, Edbrooke L,
Kiss N.
Comparison of the GLIM, ESPEN and ICD-
10 Criteria to Diagnose Malnutrition and Predict 30-Day Outcomes: An
Observational Study
in an Oncology Population.
Nutrients.
2021;13(8):2602. https://doi.org/10.3390/nu13082602
-
Tan S, Wang J, Zhou F, Tang M, Xu J, Zhang
Y, et al.
Validation of GLIM malnutrition criteria
in cancer patients undergoing major abdominal surgery: A large-scale
prospective study.
Clin Nutr. 2022;41(3):599-609. https://doi.org/10.1016/j.clnu.2022.01.010
-
Steer B, Loeliger J, Edbrooke L, Deftereos
I, Laing E, Kiss N.
Malnutrition Prevalence
according to the GLIM Criteria in Head and Neck Cancer Patients
Undergoing Cancer
Treatment.
Nutrients.
2020;12(11):3493. https://doi.org/10.3390/nu12113493
-
Engelman DT, Ben Ali W, Williams JB,
Perrault LP, Reddy VS,
Arora
RC, et al.
Guidelines for Perioperative Care in Cardiac Surgery: Enhanced
Recovery After Surgery
Society Recommendations.
JAMA Surg.
2019;154(8):75-766. https://doi.org/10.1001/jamasurg.2019.1153
-
Hill A, Arora RC, Engelman DT, Stoppe C.
Preoperative Treatment of Malnutrition and
Sarcopenia in Cardiac Surgery: New Frontiers.
Crit Care Clin.
2020;36(4):593-616. https://doi.org/10.1016/j.ccc.2020.06.002
-
Lopez-Delgado JC, Muñoz-del Rio G,
Flordelís-Lasierra JL, Putzu
A.
Nutrition in Adult
Cardiac Surgery: Preoperative Evaluation, Management in the
Postoperative Period, and
Clinical Implications for Outcomes.
J Cardiothorac Vasc Anesth.
2019;33(11):3143-3162.
https://doi.org/10.1053/j.jvca.2019.04.002