Abstract
Introduction: The premature birth of twins with bronchopulmonary
dysplasia and/or retinopathy
of prematurity represents an emotional, social, and financial challenge for families.
Objective: To
understand the lived experiences of caregivers of premature twins diagnosed with bronchopulmonary
dysplasia and retinopathy of prematurity in a Kangaroo Mother Care program in Bogotá, Colombia.
Materials and Methods: A phenomenological study was conducted with seven caregivers of
premature
twins enrolled in a Kangaroo Mother Care program between 2020 and 2022. Virtual semi-structured
interviews were transcribed and analyzed using content analysis, identifying thematic categories such
as emotional experiences, access to health services, and family reorganization. Ethical considerations
and confidentiality were ensured. Results: Three main categories emerged: emotional
experience,
caregiving challenges, and socioeconomic impact. The latter included reconfiguring family roles,
financial burden, and coping strategies such as community support. Discussion: The
experience of
caregivers of premature twins with chronic conditions reveals a multidimensional burden that calls
for comprehensive, family-centered care models with ongoing interdisciplinary support and public
policies that strengthen the resilience and sustainability of caregiving. Conclusion:
The importance of
an interdisciplinary, family-centered, and humanized approach to neonatal care is emphasized. Future
research should expand the sample and explore targeted interventions for this population.
Keywords: Twins; Premature Birth; Retinopathy of Prematurity;
Bronchopulmonary Dysplasia;
Caregivers.
Resumen
Introducción: El nacimiento prematuro de gemelos con displasia
broncopulmonar y/o retinopatía del prematuro representa un desafío
emocional, social y económico para las familias. Objetivo: Comprender
las experiencias vividas de cuidadores de gemelos prematuros
diagnosticados con displasia broncopulmonar y retinopatía en el
contexto de un Programa Madre Canguro en Bogotá, Colombia.
Materiales y Métodos: Se realizó un estudio fenomenológico con
siete cuidadores de gemelos prematuros participantes en el Programa
Madre Canguro entre 2020 y 2022. Las entrevistas semiestructuradas
virtuales se transcribieron y analizaron mediante análisis de contenido,
identificando categorías temáticas como experiencia emocional,
acceso a servicios de salud y reorganización familiar. Se aseguraron
aspectos éticos y confidencialidad. Resultados: Emergieron tres
categorías principales: Experiencia emocional, desafíos en el cuidado
e impacto socioeconómico: Reconfiguración de roles familiares, carga
económica y estrategias de afrontamiento como el apoyo comunitario.
Discusión: La experiencia de cuidadores de gemelos prematuros con
patologías crónicas revela una carga multidimensional que demanda
modelos de atención integrales, centrados en la familia, con apoyo
interdisciplinario continuo y políticas públicas que fortalezcan la
resiliencia y sostenibilidad del cuidado. Conclusión: Se destaca la
importancia de un enfoque interdisciplinario y humanizado en la
atención neonatal, centrado en las familias. Futuras investigaciones
deberían ampliar la muestra y explorar intervenciones específicas para
esta población.
Palabras Clave: Gemelos; Nacimiento Prematuro; Retinopatía de la
Prematuridad; Displasia Broncopulmonar; Cuidadores.
Resumo
Introdução: O nascimento prematuro de gêmeos com displasia
broncopulmonar e/ou retinopatia
da prematuridade representa um desafio emocional, social e econômico para as famílias.
Objetivo:
Compreender as experiências vividas por cuidadores de gêmeos prematuros diagnosticados com displasia
broncopulmonar e retinopatia no contexto de um Programa de Cuidado Materno Canguru em Bogotá,
Colômbia. Materiais e Métodos: Foi realizado um estudo fenomenológico com sete
cuidadores de gêmeos
prematuros participantes do Programa de Cuidado Materno Canguru entre 2020 e 2022. Entrevistas
virtuais semiestruturadas foram transcritas e analisadas por meio de análise de conteúdo, identificando
categorias temáticas como experiência emocional, acesso a serviços de saúde e reorganização familiar.
As considerações éticas e a confidencialidade foram asseguradas. Resultados: Três
categorias principais
emergiram: experiência emocional, desafios do cuidado e impacto socioeconômico: reconfiguração
dos papéis familiares, ônus econômico e estratégias de enfrentamento, como o apoio da comunidade.
Discussão: A experiência dos cuidadores de gêmeos prematuros com doenças crônicas
revela um
fardo multidimensional que exige modelos de cuidado abrangentes e centrados na família, com apoio
interdisciplinar contínuo e políticas públicas que fortaleçam a resiliência e a sustentabilidade do
cuidado.
Conclusão: Destaca-se a importância de uma abordagem interdisciplinar e humanizada para
o cuidado
neonatal, centrada nas famílias. Pesquisas futuras devem ampliar o tamanho da amostra e explorar
intervenções específicas para essa população.
Palavras-Chave: Gêmeos; Nascimento Prematuro; Retinopatia da
Prematuridade; Displasia
Broncopulmonar; Cuidadores.
Introduction
Premature birth is a complex event that poses multiple challenges for the newborn
and the family.
Each year, approximately 15 million infants are born prematurely, making it one of the leading
causes
of neonatal morbidity and mortality worldwide1. Among the most common complications are
bronchopulmonary dysplasia (BPD) and retinopathy of prematurity (ROP), which may result in
longterm
respiratory and visual impairments and require specialized medical follow-up2,3.
Caring for a child with BPD and/or ROP entails a significant emotional, social,
and financial impact on
the family, due to prolonged hospitalizations, complex treatments, and uncertainty regarding
their
children’s development4. Parents of preterm infants experience high
levels of stress, anxiety, and
depression, arising from their children’s vulnerability and the need to assume an active
caregiving
role5- 7.
Studies report that approximately 40% of parents experience depressive symptoms and
around 50% experience anxiety symptoms in the immediate period following premature birth, while
up to three-quarters report high levels of overall stress8, 9. This burden is intensified in the case of
premature twins, as caregiving demands are doubled and challenges in family organization and
access to support resources increase10.
Early intervention programs, such as Kangaroo Mother Care (KMC), have shown benefits for
the
prognosis of preterm infants and for strengthening parenting11. However,
evidence on their impact
on families of twins with BPD and/or ROP is limited. Previous literature has primarily
focused on the
mother-infant relationship and psychosocial risk factors, overlooking the experience of
simultaneously
caring for two children with complex chronic conditions, the challenges of family
reorganization,
and the levels of stress this entails12.
Furthermore, it is essential to understand how family members
experience the transition from hospital to home and which coping strategies they develop
to manage
the emotional and logistical burden of care.
From a phenomenological perspective, exploring the experiences of these
caregivers provides insights
into the meanings they ascribe and their needs for emotional, social, and health care
support in this
context. Accordingly, this study aimed to understand the experiences of caregivers of
premature
twins with bronchopulmonary dysplasia and retinopathy of prematurity in a Kangaroo
Mother Care
program in Bogotá, Colombia.
Materials and Methods
Study design
A qualitative study with a phenomenological approach was conducted to understand the
experiences
of caregivers of twins with BPD and/or ROP enrolled in a KMC program in Bogotá between
2020 and
2022. This approach enabled the exploration of the meanings underlying their lived
experiences13.
As this was a qualitative study, the Consolidated Criteria for Reporting Qualitative
Research (COREQ)
guidelines were followed14.
The sample consisted of seven caregivers of premature twins, selected through
convenience sampling
supported by the program guidelines, based on their experience and eligibility.
Inclusion criteria were
caregivers aged 18 years or older; infants born at less than 37 weeks’ gestation; and
active participation
in the KMC program for 3 to 24 months. Finally, caregivers of children with cognitive
impairments,
congenital malformations, special needs, or health conditions that could limit
participation were
excluded, as well as those who declined to participate in the study.
Data collection
Data were collected between 2020 and 2022, a period marked by the pandemic, which led to
significant
adjustments in the KMC program. Caregivers were initially contacted by telephone, and
the study
was briefly introduced, and potential risks were explained. All family members agreed to
participate
voluntarily. Subsequently, semi-structured interviews were conducted, with questions
adapted to
caregivers’ level of understanding to explore their emotional life experiences,
caregiving experiences,
and the difficulties encountered during the process. The average duration of each
interview was 45
minutes.
A total of seven virtual interviews were conducted by the principal investigator, who
has extensive
experience in the comprehensive care of preterm infants and their families. No pilot
testing was
conducted, nor was it necessary to repeat interviews, as the accounts obtained were
sufficient for the
analysis and understanding of the phenomenon under study.
Data analysis
The interviews were audio-recorded, transcribed verbatim, and shared with participants,
who returned
them without requesting any modifications. Data were managed using ATLAS.ti software.
Data
analysis followed Bardin’s content analysis approach through an inductive process that
included
the phases of pre-analysis, coding, and categorization15, 16. Coding was performed independently
by two co-investigators, who conducted iterative readings of the transcripts to identify
relevant
meaning units. Subsequently, a hierarchical coding tree was developed from codes
formulated as
interpretive expressions, which condensed the shared meanings identified in the accounts
and
facilitated the organization of the material into subcategories and categories. These
categories
enabled the identification of recurring patterns and, in turn, their grouping into core
categories that
comprehensively explained the overall experience, as presented in the Results section.
Themes were
derived inductively, emerging directly from the discourse until theoretical saturation
was reached
in the seventh interview, when redundancy in the accounts and a deep understanding of
the
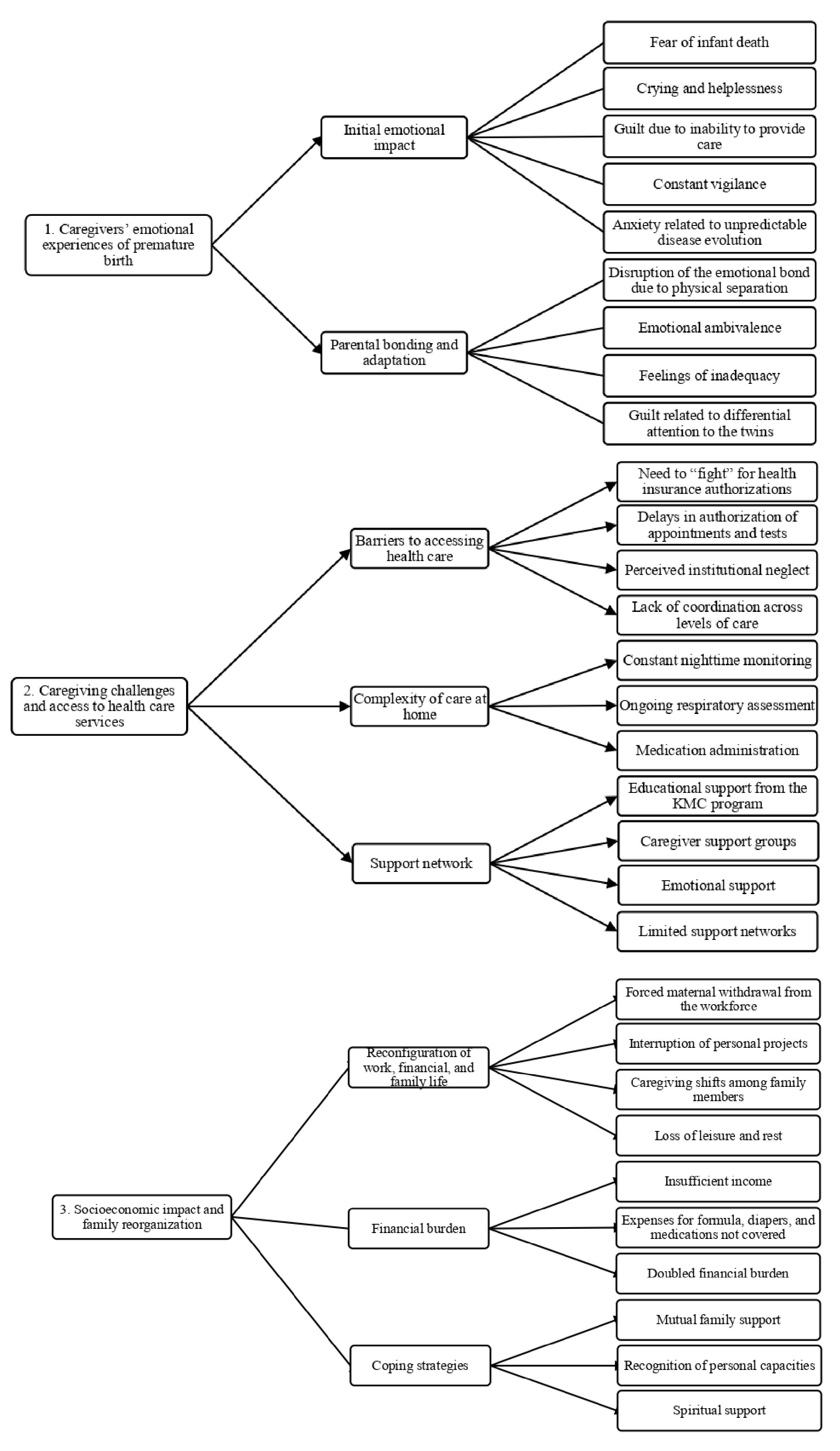
phenomenon under study became evident, as shown in Figure 1.
To ensure confidentiality, participants were identified using codes (P1,
P2, P3, and so on). For
triangulating qualitative data, the literature review and semi-structured interviews
were used as
complementary data sources. Methodological triangulation allowed comparison of emerging
findings
from caregivers’ accounts with existing theoretical knowledge on the experience of
caregiving in
preterm multiple births, thereby strengthening the credibility and trustworthiness of
the results.
Although observation diaries were initially considered as a third source of
triangulation, pandemicrelated
constraints precluded their inclusion; therefore, greater emphasis was placed on
comparative
analysis between the primary data and the specialized literature. To ensure
confidentiality, the
accounts were coded and organized into an anonymized qualitative dataset, available in
Mendeley
Data17.
Ethical considerations
In accordance with Resolution 8430 of 1993 issued by the Colombian Ministry of Health,
this study
was classified as minimal risk, as participants could experience discomfort or emotional
distress18.
Ethical approval was obtained from the Research Ethics Committee of the Subred
Sur
(approval No.
238-10032023). Following participants’ verbal agreement, informed consent was obtained,
ensuring
opportunities to address any questions.
Figure 1. Hierarchical coding tree
Results
Seven caregivers of premature twins (parents and grandmother) were interviewed,
with ages ranging
from 20 to 53 years. Of these, 85.71% (n=6) were in socioeconomic stratum 1 (the lowest level in
Colombia’s socioeconomic classification system), 71.42% (n=5) lived in rented housing, and 100%
(n=7)
reported having support networks. The number of prenatal care visits ranged from 2 to 10 Table 1.
Table 1. Individual characteristics of study participants
X
Table 1. Individual characteristics of study participants
| Code |
Kinship |
Age
(years) |
Education |
Occupation |
Socioeconomic
stratum |
Housing |
Prenatal
care visits |
Support
network |
| P1 |
Mother |
29 |
Incomplete
primary education |
Homemaker |
2 |
Rented |
6 |
Yes |
| P2 |
Mother |
24 |
Incomplete
secondary education |
Informal vendor |
1 |
Rented |
2 |
Yes |
| P3 |
Mother |
38 |
Incomplete
primary education |
Homemaker |
1 |
Rented |
10 |
Yes |
| P4 |
Mother |
20 |
Incomplete
secondary education |
Student |
1 |
Rented |
2 |
Yes |
| P5 |
Grandmother |
52 |
Incomplete
primary education |
Homemaker |
1 |
V |
Not applicable |
Yes |
| P6 |
Mother |
33 |
Incomplete
primary education |
Homemaker |
1 |
Owned |
5 |
Yes |
| P7 |
Father |
53 |
Incomplete
primary education
|
Farmer |
1 |
Owned |
Not applicable |
Yes |
Source:
Kangaroo Mother Care Program database, Subred Sur, 2020-2022.
From the analysis, three categories and their respective subcategories emerged, derived from the
codes
identified in participants’ accounts Table 2.
Table 2. Summary of the process of category and subcategory development
X
Table 2. Summary of the process of category and subcategory development
| Theme |
Category |
Subcategory |
Code |
Caregivers’
experience
|
Parents’ emotional
experience of
premature birth
|
Initial
emotional impact
Parental bonding and
adaptation
|
Reactions of shock, fear, and distress
upon receiving the
diagnosis of extreme
prematurity.
Process of
strengthening attachment and
adapting to new
responsibilities.
|
|
Care
|
Caregiving challenges and
access to health care services
|
Barriers to accessing health care
Complejidad del
cuidado en casa
|
Difficulties accessing appointments,
transportation, and specialized services.
Management of oxygen therapy, specialized
feeding, and adjunct therapies.
|
|
Consequences
|
Socioeconomic impact and
family reorganization
|
Reconfiguration
of work,
financial, and family life
Coping strategies
|
Adaptation of routines, redistribution of
roles, and workforce withdrawal.
Ways in which
families cope with and
overcome challenges.
|
Category 1. Caregivers’ emotional experience of premature birth
The premature birth of twins with chronic conditions such as BPD and/or ROP constitutes a
disruptive
experience. Participants’ accounts reflect a transition from the expectation of a normal
pregnancy to a
complex and highly demanding medical reality. The emotions described do not follow a linear
course
but rather are intertwined and evolve.
Initial emotional impact: Parents described twin delivery and the
clinical diagnosis as a disruptive
experience, characterized by a sense of loss of control, vulnerability, fear, and distress in
the face of the
possibility of losing their children. This perceived imminent threat marked the beginning of a
complex
emotional process.
“When they told me my babies had to stay in the ICU, I felt like my world was falling
apart. I didn’t know
what to do—I just cried.” (P2)”
Infants’ body language, such as minimal movements, extreme fragility, and technological
dependence,
generated an affective shock that some caregivers described as paralyzing.
“It was really hard to see them so tiny and hooked up to all those wires. I felt
helpless, like there was
nothing I could do for them.” (P1)
Birth under these conditions initially limits parents in their role as active caregivers,
leading to feelings
of guilt, inadequacy, or uselessness that affect bonding. In multiple pregnancies, this impact
is amplified
as parents face the challenge of attending to the pain, fragility, and needs of both
infants.
“When they told me it was a high-risk pregnancy, I was really scared because they said I
had to be extremely
careful and stop working.” (P6)
In turn, the unpredictable clinical course of the twins led to a state of constant vigilance,
with limited
physical and emotional rest and a persistent climate of anxiety. In this context, participants
drew on
various emotional, spiritual, and social strategies to cope.
“At first they told me they weren’t going to make it because they were so tiny, but I
held on to hope, and
now they’re here with me.” (P7)
In summary, the initial emotional impact is expressed as acute distress, marked by the perceived
life-threatening risk to their children or grandchildren, the perceived inability to fulfill the
caregiving
role, the disruption of expectations, and entry into a highly technological hospital environment
that
depersonalizes the experience of birth, making it necessary to re-signify the meaning of being a
caregiver under extreme conditions.
Parental bonding: In preterm multiple births, parental bonding was a
progressive process marked
by emotional ambivalence. Unlike what occurs under typical conditions, parents of preterm twins
with BPD and/or ROP experienced a disruption or delay in emotional bonding due to physical
separation, the medicalization of care, and the constant fear of loss.
“At first I was afraid to hold them—they were so tiny and fragile. But little by little
I learned to trust
myself and to believe they’re strong too. I felt like I wasn’t capable, but over time I
realized they need to
feel my love and my warmth.” (P5)
The KMC program played a fundamental role in this process. Guidance and support
sessions enabled
parents to take an active role in their infants’ care, transforming fear into competence and
emotional
distance into closeness.
“When they showed us how to hold them and what to do, I felt like I was a mom again. I
wasn’t just a
bystander in the hospital anymore.” (P2)
In the specific case of twins, this process was doubled and took on distinct nuances.
Some parents
expressed concern about forming unequal bonds with each child, particularly when one twin had a
more complex clinical course than the other.
“Sometimes I paid more attention to the one who was more fragile, and then I’d feel guilty for
not being
the same with the other. You don’t want there to be any differences, but it’s hard.” (P7)
In sum, parental bonding in this context was neither immediate nor spontaneous but
rather the result
of a process of emotional reconstruction, kinesthetic learning, and redefinition of the maternal or
paternal role. Premature birth did not prevent bonding; rather, it reshaped it into more conscious,
engaged, and transformative forms.
Category 2. Caregiving challenges and access to health care services
Caring for premature twins with chronic conditions is embedded in a daily reality shaped by practical
challenges. This category captures the tensions caregivers experience in accessing healthcare, the
complexities of specialized home-based care, and how they perceive the presence or absence of
support from institutions and formal and informal networks.
Barriers to accessing health care: Participants’ accounts indicate that one of
the greatest difficulties
was timely, continuous, and effective access to healthcare services. The barriers identified were
related not only to structural shortcomings of the system but also to a subjective experience of
abandonment, invisibility, and emotional strain.
“We’ve had to fight with the insurance company to get authorizations. If you don’t push, they
don’t do
anything.” (P2)
Caregivers reported that specialist appointments, diagnostic tests, and required therapies were
not
scheduled promptly, as needed. These delays were perceived as a direct risk to the infants’
health,
generating anxiety and feelings of helplessness.
“Sometimes they’d give me appointments way too late, and I had to keep pushing to get
them seen
sooner because they can’t wait that long.” (P4)
Access barriers also included logistical challenges, such as transportation to attend
appointments,
particularly for infants dependent on oxygen or with medically fragile conditions. In
contexts of
financial vulnerability, these limitations were exacerbated by the inability to cover
associated costs,
compromising adherence to follow-up care.
Complexity of care at home: Hospital discharge of preterm
twins marked, for caregivers, the
beginning of a new phase characterized by high demands, fears, and highly specialized
responsibilities.
Participants’ accounts show that the home, rather than being a place of rest and safety,
became an
extension of the clinical setting.
“It’s really hard. You have to keep an eye on the oxygen, make sure it doesn’t
come loose, make sure
they’re eating well. You never really sleep peacefully.” (P1)
Parents assumed the role of specialized caregivers without prior professional training.
Handling medical
devices, such as oxygen cylinders, nasal cannulas, or inhalers, and administering
medications with strict
dosing and schedules became part of the daily routine, keeping a constant state of
alertness.
“I’m scared that something could happen at any moment and I wouldn’t know what
to do. Every night I
check that they’re breathing okay—I don’t sleep.” (P4)
This continuous vigilance had a significant impact on caregivers’ physical and mental
health, with
reports of exhaustion and persistent anxiety about the possibility of an emergency
occurring at home
without being able to respond in time. This fear was compounded by the need to care for
two infants
with different needs simultaneously, doubling the demands and caregiving burden.
“After the hospitalization, one of them needed oxygen for two months. It was
really hard because he
needed more attention. The other baby was doing better, but if one got sick, I’d
end up neglecting the
other.” (P3)
Despite these challenges, caregivers established routines, learned through observation,
relied on family
support networks, and developed practical, everyday knowledge that enabled them to
sustain their
infants’ lives. Participants’ accounts indicate that the close, educational support
provided by the KMC
team was key to strengthening confidence in home-based care by providing technical
knowledge,
building confidence, and fostering a sense of not being alone in facing this challenge.
“It helped us a lot that a nurse from the program explained every step. Without
that support, we wouldn’t
have known what to do.” (P6)
In addition to the healthcare team, participants identified other sources of emotional
and practical
support that were essential for sharing responsibilities, providing emotional support,
and offering
resources such as food or transportation assistance.
“In the support group, I met other moms going through the same thing. It made
me feel like I wasn’t
alone, like others were dealing with it too.” (P3)
However, support was not uniform. Some parents reported feeling alone, with insufficient
support
from the health system or limited family networks. This situation highlighted that
access to emotional
and practical support is shaped by structural factors, including socioeconomic status,
available support
networks, and institutional responsiveness.
Category 3. Socioeconomic impact and family reorganization
This category encompasses the adaptations and trade-offs families experience at the
financial and
household levels, where caregiving requires the redistribution of roles, changes in
routines, and a
reduction in household income.
Reconfiguration of work and family life: The premature birth
of twins with chronic conditions
entailed a profound transformation of work and domestic dynamics. This was not a simple
adjustment
but a rupture with the previous way of life, requiring difficult decisions, personal
sacrifices, and a
reorganization of roles centered on the care of the children.
“I had to quit my job because there was no one to take care of them. Now we’re
living on just one income,
and it’s been really hard.” (P2)
Mothers, in most cases, assumed a central caregiving role, which involved leaving their
jobs,
interrupting their studies or personal activities, and dedicating themselves exclusively
to the twins’
care.
“Before I knew it was a high-risk pregnancy, I worked for two months, but I had
to stop for my health
and the babies’. My husband has two jobs and can’t help me with the kids, so my
mom is the one who
helps me.” (P3)
Family daily life was disrupted by routines centered on the twins’ medical needs.
Household tasks,
relationships with other children, rest, and leisure were reconfigured or disappeared.
The home was
transformed into a therapeutic and highly monitored space, where each family member had
to adapt
to a new order shaped by the infants’ fragility.
“My wife and I had to figure out a schedule to take turns at the hospital and at
home, but it ended up
affecting our finances.” (P7)
At the same time, caring for two infants resulted in a sustained financial burden,
intensified by the
complexity of providing simultaneous care. This burden involved not only increased
financial costs
but also persistent financial strain, where the fear of being unable to meet needs
coexisted with an
unconditional commitment to ensuring the children’s survival and well-being.
“The money just isn’t enough. The diapers, the special formula, the medications…
it’s too much, and
sometimes we don’t know how we’re going to pay for it.” (P2)
The main sources of expenditure reported by participants included specialized formula,
large
quantities of diapers, frequent transportation to medical appointments and hospitals,
medications
not covered by health insurance, adjunct therapies, follow-up tests, and minor home
modifications
to ensure safe conditions.
“We spend everything on the treatments, and even though some things are covered,
there’s still a lot we
have to pay for ourselves.” (P1)
In sum, the financial burden of caring for premature twins with BPD and/or ROP emerges as a
factor
that exacerbates family vulnerability, undermines emotional stability, and highlights the
need for
public policies responsive to the complexity of these situations.
Coping strategies: This subcategory illustrates how families
strengthen their capacity to cope with
the challenges of having a newborn with special health care needs. Mutual support and
solidaritybased
networks became spaces for emotional support and practical assistance, facilitating more
effective coping with stress and uncertainty.
“We’ve learned to be strong as a family. We support each other a lot, and also connect
with other moms
in the program.” (P5)
Participants’ accounts indicate a process of personal and family transformation in which
families
initially feel overwhelmed and vulnerable but, over time, come to recognize their inner strength
and collective capacity to overcome challenges. This resilient growth becomes a source of hope
and
motivation to move forward despite difficulties.
“At first I didn’t think I could handle this, but now I see how far we’ve come and
realize we’re stronger
than we ever imagined.” (P6)
This strengthening process not only improves families’ quality of life but also fosters a deep
sense of
hope and empowerment. Thus, coping strategies and mutual support are consolidated as essential
pillars in the path toward emotional recovery and overall well-being of families in the context
of
specialized neonatal care.
Discussion
The findings of this study provide an in-depth understanding of the lived experiences of
caregivers
of premature twins with BPD and/or ROP. These chronic and complex conditions impose a significant
burden not only on the health of the newborns but also on the emotional, social, and financial
domains of family life4.
The process of parental bonding emerges as a dynamic and ambivalent phenomenon in which
hope is intertwined with fear and guilt, shaping a complex emotional landscape that affects family
adaptation5,9. The convergence of preterm
multiple births with severe conditions amplifies uncertainty
and stress, requiring parents to manage the intensive care of two children in highly medicalized
hospital settings19. This
situation increases psychological and emotional vulnerability, as previously
documented, and is further expanded here by highlighting the specific features of parental bonding
in twins and the affective demands it entails20, 21
The KMC program emerges as a key strategy to facilitate early contact and active
parental involvement,
promoting bonding and caregiving competence11. However, caring for twins requires specific
adaptations to ensure balanced care and to avoid disparities in bonding or caregiving. This aspect
warrants greater attention in clinical practice and future research.
Uncertainty, perceived as a constant source of stress, is addressed through strategies
that include
spiritual and family support, as well as communication with health care professionals22. This
multifaceted coping strengthens resilience and adaptive capacity, facilitating the management of
prolonged neonatal care. However, limited access to psychosocial services and fragmented care
create significant gaps, exacerbating isolation and vulnerability. This finding is consistent with
previous reports that underscore the need for interdisciplinary, continuous programs integrating
emotional, social, and clinical support23.
At a structural level, participants’ accounts indicate barriers to accessing quality
health care, including
delays in scheduling appointments, lack of coordination across levels of care, and lack of
individualized
follow-up24. These obstacles
reflect systemic issues that hinder continuity of care, which is essential
in BPD and ROP due to the need for regular monitoring and specialized treatments. The perceived
lack of support and the ongoing struggle to access basic healthcare services highlight the need to
strengthen health systems through family-centered models that ensure humanized, coordinated,
and comprehensive care, addressing both clinical and psychosocial needs21.
Likewise, preterm multiple births profoundly affect family structure and dynamics,
requiring a
reorganization of roles and responsibilities that, in many cases, entails significant financial and
social
sacrifices. Job loss, increased direct and indirect costs, and adaptations within the home reflect the
absence of adequate social support and of public policies that recognize the magnitude of these
burdens. These findings are consistent with international studies indicating that premature birth can
destabilize family well-being and lead to long-term consequences for caregivers’ quality of life. In
this
regard, health programs should incorporate mechanisms for financial support, alternative caregiving
services, and psychological support to alleviate family burden and promote the sustainability of the
caregiving environment25
26.
Finally, the findings of this study provide valuable insights for clinical practice and
the development
of public policies aimed at improving the quality of life of families of preterm infants with complex
conditions. The need for an interdisciplinary approach is emphasized, integrating clinical management,
emotional and social support, and adapting programs such as KMC to address the specific needs
of preterm multiple birth27.
In addition, the importance of future research is highlighted to explore
family experiences across diverse cultural and socioeconomic contexts and to evaluate interventions
designed to strengthen resilience and long-term well-being28.
This study has limitations that should be considered when interpreting the findings. The
small
sample size and recruitment from a single KMC program in Bogotá limit the transferability of the
results to other cultural, institutional, or socioeconomic contexts. In addition, virtual data
collection
during the pandemic restricted the observation of nonverbal cues important for phenomenological
interpretation. Finally, as a cross-sectional study focused on a specific point in the caregiving
process,
it did not allow exploration of changes in parental bonding or the sustainability of coping strategies
over time5, 6.
Conclusions
The experience of family members of twins with bronchopulmonary dysplasia and retinopathy
of
prematurity reveals a complex clinical, emotional, and social burden. Although the Kangaroo Mother
Care program strengthens parental bonding and caregiving, it requires adaptations to address the
demands of simultaneous care. Barriers to access, along with the lack of psychosocial and financial
support, increase family vulnerability, underscoring the need to strengthen health systems through
comprehensive, family-centered approaches and to advance public policies and research that address
these needs.
Finally, this study reaffirms the central role of the interdisciplinary neonatal health
care team in the
comprehensive, humanized care of premature twins with chronic conditions and their families. Their
role extends beyond clinical and technical tasks to include emotional support, caregiver education,
and the coordination of support networks. The findings highlight these professionals as key actors
in the consolidation of family-centered care models, capable of responding to the complexity of
preterm multiple births and contributing significantly to improving the quality of life of both the
newborns and their families.
Conflicts of Interest: The authors declare no conflicts of interest
related to this study.
Funding: The research was approved under the internal research call at
Areandina in 2023 and was
supported by institutional resources under code CV2023-CSD-B-12935.
Author contributions: SEGS: Conceptualization; Methodology;
Investigation; Project Administration;
Supervision; Validation; Writing- original draft; Writing – review & editing. NCH: Data curation;
Investigation; Formal analysis; Visualization; Writing- original draft; Software; Writing – review
& editing. AMMG: Data curation; Investigation; Formal analysis; Visualization; Writing- original
draft; Software; Writing – review & editing. OMN-R: Conceptualization; Methodology; Supervision;
Validation; Resources; Writing – review & editing. GJC-M: Conceptualizatiin; Methodology; Supervision;
Validation; Resources; Software; Writing – review & editing. RLL-C: Conceptualization; Methodology;
Supervision; Validation; Resources; Writing – review & editing.
References
-
World Health Organization. Preterm birth. 2023. Cited: 2025
March 9. Available from:
https://www.who.int/es/news-room/fact-sheets/detail/preterm-birth
-
Srivatsa B, Malcolm K, Clark RH, Kupke KG. Effect of a Novel
Oxygen Saturation Targeting
Strategy on Mortality, Retinopathy of Prematurity, and Bronchopulmonary Dysplasia in
Neonates Born Extremely Preterm. J Pediatr.
2021;234:33-37.e3.
https://doi.org/10.1016/j.jpeds.2021.03.007
-
Singh JK, Wymore EM, Wagner BD, Thevarajah TS, Jung JL, Kinsella JP, et
al.
Relationship
between severe bronchopulmonary dysplasia and severe retinopathy of prematurity
in premature newborns.
J AAPOS.
2019;23(4):209.e1-209.e4.
https://doi.org/10.1016/j.jaapos.2019.02.008
-
Pérez Pérez G, Navarro Merino M.
Displasia broncopulmonar y prematuridad. Evolución
respiratoria a corto y a largo plazo. An Pediatr. 2010;72(1).
https://doi.org/10.1016/j.anpedi.2009.09.010
-
Osorio Galeano SP, Salazar Maya AM. El empoderamiento de los
padres para el cuidado del
hijo prematuro.
Rev Cuid.
2022;13(2) http://dx.doi.org/10.15649/cuidarte.2104
-
Nyaloko MJ, Lubbe W, Moloko-Phiri SS, Shopo KD.Parental
experiences of caring for
preterm infants in the neonatal intensive care unit, Limpopo Province: a descriptive qualitative
study exploring the cultural determinants.
BMC Health Serv Res. 2024;24:669. https://doi.org/10.1186/s12913-024-11117-6
-
Furtak SL, Gay CL, Kriz RM, Bisgaard R, Bolick SC, Lothe B, et
al. What parents want to
know about caring for their preterm infant: A longitudinal descriptive study. Patient Educ
Couns. 2021;104(11):2732-2739. https://doi.org/10.1016/j.pec.2021.04.011
-
Vigod SN, Villegas L, Dennis CL, Ross LE. Prevalence and risk
factors for postpartum
depression among women with preterm and low-birth-weight infants: a systematic review. An
International Journal of Obstetrics & Gynaecology.
2010;117(5):540-550. https://doi.org/10.1111/j.1471-0528.2009.02493.x
-
Shaw RJ, Deblois T, Ikuta L, Ginzburg K, Fleisher B, Koopman C.
Acute stress disorder among
parents of infants in the neonatal intensive care nursery. Psychosomatics.
2006;47(3):206-212.
https://doi.org/10.1176/appi.psy.47.3.206
-
Freitas MJ, Maneta Travanca IS, García-Fernández R. Parents’
Needs When Experiencing
the Transition to Twin Parenthood. Healthcare.
2024;12(12). https://doi.org/10.3390/healthcare12121173
-
Lizarazo-Medina JP, Ospina-Diaz JM, Ariza-Riaño NE.
Programa madre canguro: una
alternativa sencilla y costo eficaz para la protección de los recién nacidos prematuros o
con bajo peso al nacer.
Rev Salud Publica.
2013;14(2):32–45. https://www.scielosp.org/pdf/rsap/2012.v14suppl2/32-45/es
-
Beer C, Israel C, Johnson S, Marlow N, Whitelaw A, Glazebrook
C.
Twin birth: an additional
risk factor for poorer quality maternal interactions with very preterm infants?.
Early Hum Dev. 2013;89(8):555-559. https://doi.org/10.1016/j.earlhumdev.2013.02.006
-
Fuster Guillen DE.
Investigación cualitativa: Método fenomenológico hermenéutico. Propósitos y
Representacioned. 2019;7(1):201-229. http://dx.doi.org/10.20511/pyr2019.v7n1.267
-
Simister R, Black GB, Melnychuk M, Ramsay AIG, Baim-Lance A, Cohen DL,
et al.
Temporal
variations in quality of acute stroke care and outcomes in London hyperacute stroke units:
a mixed-methods study.
Health Soc Deliv Res.
2020;8(34). https://doi.org/10.3310/hsdr08340
-
Bardin L. Análise de conteúdo. 1 Ed. Edições 70, editor. São
Paulo; 2016. 279 p.
-
Soratto J, Pires DEP, Friese S.
Thematic content analysis using ATLAS.ti software: Potentialities
for researchs in health. Rev Bras Enferm.
2020;73(3):e20190250 https://doi.org/10.1590/0034-7167-2019-0250
-
Guevara-Suta S, Hernández Casallas N.
“Experiencias de familiares de gemelos con displasia
broncopulmonar y retinopatía: estudio fenomenológico”,
Mendeley Data, V1. 2025.
https://doi.org/10.17632/gnppjxd2rn.1
-
Ministerio de Salud y Protección Social. Resolución 8430 de
1993: Por la cual se establecen
las normas científicas, técnicas y administrativas para la investigación en salud. p. 471–3.
Bogotá: 1993.
-
Ishida S, Nakanishi H, Sekiya R, Kawada K, Kosaka Y, Yamaguchi A, et
al.
Impact of lateonset
circulatory collapse and bronchopulmonary dysplasia on short-term outcomes in
preterm infants: A Japanese retrospective cohort study.
Pediatr Neonatol. 2025;66(5):462-466. https://doi.org/10.1016/j.pedneo.2024.08.006
-
Barra CL, Marín P, Coo S. Developmental care of premature
newborns: Fundamentals and
main characteristics.
Andes Pediatr. 2021;92(1):131-137. https://pubmed.ncbi.nlm.https://pubmed.ncbi.nlm.nih.gov/34106194/nih.gov/34106194/
-
Tung YL, Chu SM, Lien R, Fu RH, Hsu KH, Chiang MC, et al. PA
comprehensive analysis of
clinical variables for severe bronchopulmonary dysplasia in extremely preterm infants.
Pediatr
Neonatol. 2025;66(5):478-483.
https://doi.org/10.1016/j.pedneo.2025.01.006
-
Bolivar Montes LA, Montalvo Prieto A. Uncertainty associated to
parents of preterm infants
hospitalized in neonatal intensive care units. Investig y Educ en Enferm. 2016;34(2).
https://doi.org/10.17533/udea.iee.v34n2a16
-
Querido D, Lourenço M, Charepe Z, Caldeira S, Nunes E.
Nursing interventions concerning
the bonding of hospitalized newborns – scoping review. Enferm Glob.
2022;21(2):594-637.
https://dx.doi.org/10.6018/eglobal.479291
-
Heinonen K.
Listening to the Fathers of Twins—Being Sensitive to Fathers’ Needs in
Maternity and Child Healthcare.
Int J Environ Res Public Health.
2022;19(17):10639.
https://doi.org/10.3390/ijerph191710639
-
Bolch CE, Davis PG, Umstad MP, Fisher JRW. Multiple birth
families with children with
special needs: A qualitative investigation of mothers’ experiences.
Twin Res Hum Genet. 2012;15(4):503-515. https://doi.org/10.1017/thg.2012.24
-
Wenze SJ, Battle CL, Tezanos KM.
Raising multiples: mental health of mothers and fathers
in early parenthood.
Arch Womens Ment Health.
2014;18:163-176.
https://doi.org/10.1007/s00737-014-0484-x
-
González MA, Alfie J.
Una revisión acerca del cuidado de la salud mental en las familias de
la Unidad de Cuidados Intensivos Neonatales.
Rev del Hosp Ital B.Aires. 2023;43(3):134-138. https://doi.org/10.51987/revhospitalbaires.v43i3.270
-
Peña Silva B, García Araya A, Miranda Iglesias M, Caviedes Fernández J,
Ulloa Ramírez
V, Rementería Rementería Y.
Estrés parental y sus dimensiones en Unidades de Cuidado
Intensivo Neonatal – Pediátrica: Revisión Narrativa. ACC CIETNA.
Rev la Esc Enfermería. 2021;8(2):67-84. https://doi.org/10.35383/cietna.v8i2.611