Rev Cuid. 2025; 16(3): e5800
Abstract
Introduction:
Population aging and the rise in chronic diseases demand strengthening strategies to promote the well-being of institutionalized older adults. The FUMAT scale enables the assessment of quality of life across eight dimensions of well-being.
Objective:
To analyze the factors associated with the quality-of-life profile of institutionalized older adults.
Material and Methods:
A cross-sectional analytical study was conducted with 250 permanent residents (≥3 months) of a nursing home in Bucaramanga, Colombia. Individuals aged 60 years or older with a reliable informant were included; those with terminal illness, acute psychiatric disorders, or clinical instability were excluded. The FUMAT scale, Barthel Index, PULSES profile, FRAIL scale, Downton Fall Risk Index, and the Short Portable Mental Status Questionnaire (SPMSQ) were applied. Descriptive and bivariate analyses were performed using Pearson's chi-square test, Fisher’s exact test, and the Mann–Whitney U test. Multivariate analysis was conducted using binary logistic regression. Data were processed using Stata v17.
Results:
The lowest-scoring dimensions were material well-being and interpersonal relationships, whereas rights and social inclusion achieved the highest scores. Physical activity and participation in productive activities were associated with better scores on the FUMAT Quality-of-Life Index (FUMAT-QOLI). In the multivariate model, cognitive impairment (OR=0.34; 95% CI: 0.12–0.91) and motor impairment (OR=0.30; 95% CI: 0.14–0.64) significantly reduced the likelihood of belonging to the highest FUMAT-QOLI tertile; physical and productive activities showed a positive but non-significant trend.
Discussion:
The findings indicate that functional capacity and cognitive integrity are key determinants of well-being among institutionalized older adults. Low scores in material well-being and interpersonal relations suggest resource and social support limitations, requiring institutional intervention. The association between activity and well-being supports the implementation of active aging programs.
Conclusion:
Promoting autonomy, cognitive stimulation, and social integration is essential to improve quality of life.
Keywords:
Quality of Life; Aged; Institutionalization; Geriatric Nursing; Physical Activity.
Resumen
Introducción:
El envejecimiento y el aumento de enfermedades crónicas exigen fortalecer estrategias que promuevan el bienestar de las personas mayores institucionalizadas. La escala FUMAT permite evaluar la calidad de vida a partir de ocho dimensiones del bienestar.
Objetivo:
Analizar los factores asociados al perfil de calidad de vida en personas mayores institucionalizadas.
Materiales y Métodos:
Estudio transversal analítico con 250 residentes permanentes (≥3 meses) de un centro gerontológico en Bucaramanga, Colombia. Se incluyeron personas de 60 años o más con informante confiable; se excluyeron quienes presentaron enfermedad terminal, trastornos psiquiátricos agudos o inestabilidad clínica. Se aplicaron la escala FUMAT, el índice de Barthel, el PULSES profile, la escala FRAIL, el índice de riesgo de caída Downton y el Short Portable Mental Status Questionnaire (SPMSQ). Se realizaron análisis descriptivos y bivariados mediante las pruebas chi-cuadrado de Pearson, exacta de Fisher y U de Mann-Whitney. Para el análisis multivariado se utilizó regresión logística binaria. Los datos fueron procesados en Stata v17.
Resultados:
Las dimensiones con menores puntajes fueron bienestar material y relaciones interpersonales, mientras que derechos e inclusión social obtuvieron los valores más altos. La actividad física y la participación productiva se asociaron con mejores puntajes del Índice de Calidad de Vida FUMAT (ICV-FUMAT). En el modelo multivariado, la discapacidad cognitiva (OR=0.34; IC95%: 0.12–0.91) y la discapacidad motora (OR=0.30; IC95%: 0.14–0.64) redujeron significativamente la probabilidad de pertenecer al tercil superior del índice; la actividad física y productiva mostró tendencia positiva sin significancia.
Discusión:
Los hallazgos evidencian que la funcionalidad y la integridad cognitiva son determinantes del bienestar en personas mayores institucionalizadas. Las bajas puntuaciones en bienestar material y relaciones sugieren carencias en recursos y apoyo social que requieren intervención institucional. La relación entre actividad y bienestar respalda programas de envejecimiento activo.
Conclusión:
Fomentar autonomía, estimulación cognitiva e integración social es esencial para mejorar la calidad de vida.
Palabras Clave:
Calidad de Vida; Persona Mayor; Institucionalización; Enfermería Geriátrica; Actividad Física.
Resumo
Introdução:
O envelhecimento populacional e o aumento das doenças crônicas exigem estratégias que promovam o bem-estar de idosos institucionalizados. A Escala FUMAT permite avaliar de forma abrangente a qualidade de vida a partir de oito dimensões do bem-estar.
Objetivo:
Analisar os fatores associados ao perfil de qualidade de vida de idosos institucionalizados.
Materiais e Métodos:
Estudo transversal analítico realizado com 250 residentes permanentes (≥3 meses) de um centro gerontológico em Bucaramanga, Colômbia. Foram incluídos indivíduos com 60 anos ou mais e com informante confiável; excluíram-se aqueles com doença terminal, transtornos psiquiátricos agudos ou instabilidade clínica. Foram aplicados os instrumentos: Escala FUMAT, Índice de Barthel, PULSES profile, escala FRAIL, Índice de Downton e Short Portable Mental Status Questionnaire (SPMSQ). Realizaram-se análises descritivas e bivariadas utilizando os testes Qui-quadrado, Fisher e Mann–Whitney. A análise multivariada foi conduzida por regressão logística binária. Os dados foram processados no Stata v17.
Resultados:
As dimensões com menores escores foram bem-estar material e relações interpessoais, enquanto direitos e inclusão social apresentaram os valores mais altos. A prática de atividade física e a participação em atividades produtivas associaram-se a melhores escores do Índice de Qualidade de Vida FUMAT (IQV-FUMAT). No modelo multivariado, a deficiência cognitiva (OR=0.34; IC95%: 0.12–0.91) e a deficiência motora (OR=0.30; IC95%: 0.14–0.64) reduziram significativamente a probabilidade de pertencer ao tercil superior do IQV-FUMAT; atividades físicas e produtivas mostraram tendência positiva, porém sem significância estatística.
Discussão:
Os achados indicam que a capacidade funcional e a integridade cognitiva são determinantes centrais do bem-estar de idosos institucionalizados. Baixos escores em bem-estar material e relações interpessoais revelam limitações de recursos e apoio social que requerem intervenção institucional. A associação entre atividade e bem-estar reforça o valor dos programas de envelhecimento ativo.
Conclusão:
Promover autonomia, estimulação cognitiva e integração social é essencial para melhorar a qualidade de vida.
Palavras-Chave:
Qualidade de Vida; Idoso; Institucionalização; Enfermagem Geriátrica; Atividade Física.
Introduction
Increased life expectancy and declining birth rates have led to an inversion of the population
pyramid
1.
In Colombia, the National Administrative Department of Statistics (DANE) reported a 14.6%
decline in births
2,
while projections from the World Health Organization (WHO) indicate sustained
growth in population ageing both globally and across Latin American countries
3.
This phenomenon requires that care for older adults focus not only on prolonging life, but also on ensuring optimal
living conditions. The increase in chronic diseases and the growing demand for specialized services
have reinforced the role of nursing as a fundamental axis in promoting active and dignified aging
4.
From this perspective, the study and implementation of strategies aimed at improving quality of life
become a priority, considering dimensions such as physical and emotional well-being, interpersonal
relationships, self-determination, personal development, and social inclusion
5,6.
Globally, the inversion of the population pyramid is progressing rapidly, particularly in developing
countries, resulting in aging communities
7.
This process, together with age-related physiological changes, increases the risk of falls, functional
decline, and increased mortality, thereby affecting quality of life, particularly among institutionalized individuals.
Understanding these factors is essential for nursing to design interventions that promote autonomy,
social participation, and functional and cognitive integrity
8–10.
The quality of life in later life is a multidimensional concept influenced by socioeconomic factors,
lifestyles, health, housing, and social support
11.
In Colombia, the population is undergoing rapid aging: the percentage of older adults rose from 6.9%
in 1985 to 13.8% in 2020, with projections exceeding 16% by 2030. This phenomenon is further
compounded by economic vulnerability, as only 23% receive a pension, 5% actively contribute to the
pension system, and 70% make no contributions, which, in turn, increases the risk of institutionalization
and abandonment
12.
National studies demonstrate that social support and functional capacity are determinants of quality
of life among older adults
13,
which should be understood in conjunction with environmental and cultural aspects, access to
services, personal satisfaction, and recreational activities
14.
In this context, caregivers require evidence-based training to strengthen the physical and emotional
well-being of older adults
15,
while care planning should incorporate strategies to promote physical and cognitive functioning and
social participation
16.
From an interdisciplinary approach, nursing holds a strategic position in the comprehensive
assessment and early detection of risks among institutionalized individuals
17.
In addition to providing direct care, professionals should influence public policies aimed at reducing
inequalities, ensuring access to services, and promoting social inclusion
18.
The FUMAT scale has become the standard tool for assessing quality of life in nursing homes. Based
on the model developed by Schalock and Verdugo, the scale assesses eight fundamental dimensions:
emotional well-being, physical well-being, material well-being, self-determination, personal
development, interpersonal relationships, social inclusion, and rights
6.
Its excellent psychometric properties have enabled its use in numerous studies, including one
conducted in Cúcuta, Colombia, aimed at characterizing quality-of-life profiles
19.
The scale facilitates the planning of personalized care, comprehensive monitoring of physical,
psychological, and social well-being, and identification of areas of vulnerability
20–23.
Nevertheless, the necessity persists to generate contextualized evidence that reflects the sociocultural
realities of institutional settings.
In response to this, the present study aimed to analyze the factors associated with the quality-of-life
profiles among institutionalized older adults, contributing to the design of comprehensive, ethical,
and humanized care strategies.
Materials and Methods
Design
A cross-sectional analytical study was conducted with institutionalized older adults in a nursing home
in northern Bucaramanga during 2024. The population under study consisted of users of the Albeiro
Vargas and Ángeles Custodios Foundation, which serves approximately 300 individuals from a low
socioeconomic status. The sample size (n = 250) was determined using Epidat 3.1, taking as a reference
the variability in physical well-being reported in a Spanish study (mean 44.52 ± 22.55)
24,
with an alpha error of 0.03 and a beta error of 0.80. Furthermore, the findings of Morales et al. in Ecuador
25,
which reported a 62.04% prevalence of excellent quality of life, were taken into consideration. This resulted
in an alpha error of 0.024 and a beta of 0.80.
Convenience sampling was used. Individuals aged 60 years or older were included if they were
permanent residents for at least three months and had a reliable informant. Individuals with terminal
illness, acute psychiatric disorders, or clinical instability were excluded from the study.
Data was collected by the principal investigator, a nurse in postdoctoral training, following a three-month
period of interaction and observation at the nursing home, which enabled an understanding of the
participants’ social and functional dynamics. The FUMAT scale was administered with the support of
gerontologists and caregivers, who acted as key informants to ensure the validity and reliability of the
responses. The remaining instruments were administered directly by the researcher in accordance
with standardized procedures. This methodological strategy ensured objectivity, consistency, and
accuracy, faithfully reflecting the real conditions of institutionalized older adults.
Instruments
The FUMAT scale is an instrument designed to evaluate the quality of life of older adults, including
those with severe physical disability or cognitive impairment, based on the model developed
by Schalock and Verdugo
4.
It exhibits high content validity and internal consistency (α = 0.95) and adequate reliability (r = 0.90).
Its application, intended for professionals familiar with the individual, does not require the direct
participation of the person assessed and is based on observable behaviors. The scale consists of 57
items phrased in the third person, with four response options, and assesses eight dimensions:
emotional well-being, interpersonal relationships, material well-being, personal development,
physical well-being, self-determination, social inclusion, and rights
6,26.
The scale enables the creation of an individual profile using standardized scores that are comparable
across dimensions, as well as an overall index and a percentile that reflect the level of quality of life,
with higher values indicating better well-being.
Additionally, functional assessment instruments widely used in nursing practice were employed.
The Barthel Index is a widely used instrument for assessing independence in basic activities of daily
living among individuals with functional impairment, especially older adults. The instrument has
demonstrated high reliability and validity across multiple studies, with internal consistency exceeding
0.85. The Barthel Index assesses ten basic activities and assigns scores ranging from 0 to 100, with
lower scores denoting increased dependence: 0 to 20 (total dependence), 21 to 60 (severe dependence),
61 to 90 (moderate dependence), 91 to 99 (mild dependence), and 100 (independence). This scale
enables the identification of the level of functional independence, guides care planning, and supports
the assessment of the effectiveness of interventions aimed at maintaining or restoring autonomy
27–29.
The PULSES profile assesses disability and functional status across different clinical settings, including
rehabilitation and older adult care. It examines six dimensions: physical condition, upper and lower
limb function, sensory stability, excretory function, and social and mental status. The instrument has
demonstrated high interobserver reliability (r > 0.80) and good internal consistency (α = 0.75–0.90).
Each dimension is scored on a scale from 1 (independence) to 4 (severe dependence), with a total
possible score of 6 to 24 points. Lower values indicate higher functional independence. Its comprehensive
score facilitates categorization of disability, guides clinical decisions, prioritizes interventions, and
monitors functional progression, making it a widely used instrument for planning autonomy-centered
care
30–32.
The FRAIL scale identifies frailty in older adults and enables the prediction of risks such as disability,
hospitalization, and mortality. It assesses five dimensions: fatigue, resistance, aerobic capacity,
illness, and loss of weight. Each item is scored 0 or 1, yielding a total score ranging from 0 to 5 that
classifies individuals as robust (0), pre-frail (1–2), or frail (3–5). The scale has been validated across
various geriatric populations and clinical settings, demonstrating high sensitivity, specificity, and
interobserver reproducibility
33–35.
The Downton Fall Risk Index assesses the risk of falls in older adults through five items: previous
falls, medication use, sensory deficits, mental state, and gait. Each item is scored as 0 or 1, with a
maximum total score of 5; values of 3 or higher indicate high risk. The instrument has demonstrated
good sensitivity and specificity in detecting the risk of falls in the geriatric population; however, its
clinical application has been characterized by high sensitivity and low specificity
36–38.
The Pfeiffer’s SPMSQ is a brief instrument for detecting cognitive impairment in older adults. It assesses
orientation, memory, calculation, and general knowledge through ten items administered rapidly.
The instrument demonstrated good interobserver reliability (0.73) and intraobserver reliability (0.93),
supporting its consistency. Each incorrect response is counted as an error, and the total number of
errors is used to classify cognitive impairment as follows: 0–2 errors (normal), 3–4 (mild), 5–7
(moderate), and 8–10 (severe)
39–41.
Data analysis
A descriptive analysis was performed according to the nature of the variables. Absolute and relative
frequencies were calculated for qualitative variables, while medians and interquartile ranges were
reported for quantitative variables. Distributional assumptions were assessed using the Shapiro–Francia
test. Box-and-whisker plots were generated to illustrate the percentiles of the FUMAT Quality of Life
Index (FUMAT-QOLI) dimensions.
The outcome variable, the FUMAT Quality of Life Index, was categorized into tertiles; the first and
second tertiles were grouped and compared with the third tertile, resulting in the creation of a
dichotomous nominal variable. Pearson’s chi-square test or Fisher’s exact test was used for qualitative
variables, and the Mann–Whitney U test was applied for quantitative variables.
Correlation analysis was conducted using Spearman’s rho, and a correlation matrix was generated
to examine the relationships between age and the scores of the FUMAT-QOLI, the Barthel Index,
the PULSES profile, the FRAIL scale, the Downton Fall Risk Index, and the SPMSQ.
To identify factors associated with the upper tertile of the QLI, multivariate logistic regression was
performed following the steps proposed by Hosmer and Lemeshow
42,
including variables with p < 0.05 in the bivariate analysis and age, given its clinical relevance. Model’s
fit was assessed using the Hosmer–Lemeshow test. All analyses were conducted using Stata v17 and,
in accordance with the open science guidelines, the data were deposited in Mendeley Data
43.
Ethical considerations
The research was conducted in accordance with the principles of confidentiality and data protection,
thereby ensuring that participants were the focus of ethical protection. Data collection was conducted
with only free, voluntary, informed consent, and all information was stored in protected files under the
custody of the principal investigator, thereby preserving participants’ privacy and confidentiality.
Data obtained through instruments, techniques, and interviews were used exclusively for the purposes
of the study. The nursing home provided adequate spaces that ensured privacy, confidentiality, and
compliance with biosafety standards. Participants’ rights were safeguarded in accordance with national
and international regulations, ensuring that neither healthcare staff nor the services provided were
affected during the research process. The study received approval from the Bioethics Committee, as
documented in Minutes No. 007 dated April 17, 2023.
Results
Of the 250 participants, 63.60% (n=159) were female, and 36.40% (n=91) were male, with a median
age of 77.6 years (interquartile range [IQR: 70.23–84]). Table 1 presents a comparison between
participants in the initial two tertiles of the FUMAT Quality of Life Index (FUMAT-QOLI) and those in
the third tertile (highest scores). Statistically significant age differences were identified: participants
in terciles 1 and 2 had a median age of 79.84 years (IQR: 72.38–84.95), whereas those in the third
tertile had a median age of 73.65 years (IQR: 67.86–79.23) (p < 0.001), indicating a better quality of life
among the younger age groups.
Regarding educational level, participants with no education or only primary education were mainly
concentrated in the third tertile, whereas those with secondary or professional education were
more frequently represented in tertiles 1 and 2. This suggests an association between educational
attainment and self-perceived well-being.
Regarding personal medical history, statistically significant associations (p < 0.05) were observed
among participants with psychiatric, degenerative, and respiratory diseases, as well as among those
who reported the use of tranquilizers or antidepressants. Similarly, individuals with mental, cognitive,
motor, or multiple disabilities exhibited a lower proportion among those with the highest FUMAT-
QOLI scores. Conversely, individuals who reported engaging in regular physical activity and productive
activities were concentrated in the third tertile, supporting the positive relationship between active
aging and the perception of a better quality of life.
Table 1. Comparison of FUMAT-QOLI tertiles with participant characteristics
X
Table 1. Comparison of FUMAT-QOLI tertiles with participant characteristics
| Characteristics |
Total % (n)
(250) |
Tertiles 1/2 lower level
7–76 (171) |
Tertile 3 higher level
77–93 (79) |
p-value |
| Sex |
| | | 0.573 |
| Female |
63.60 (159) |
64.91 (111) |
60.76 (48) |
|
| Male |
36.40 (91) |
35.09 (60) |
39.24 (31) |
|
| Age, median (IQR) |
77.60 [70.23; 84.00] |
79.84 [72.38; 84.95] |
73.65 [67.86; 79.23] |
<0.001 |
| Marital status |
| | | 0.852 |
| Married/Cohabiting |
25.15 (43) |
25.15 (43) |
24.05 (19) |
|
| Single/Divorced/Widowed |
74.85 (128) |
74.85 (128) |
75.95 (60) |
|
| Level of education |
| | | 0.002 |
| None |
25.60 (64) |
22.22 (38) |
32.91 (26) |
|
| Primary education |
55.20 (138) |
52.63 (90) |
60.76 (48) |
|
| Secondary education |
8.80 (22) |
11.11 (19) |
3.80 (3) |
|
| Professional education |
3.60 (9) |
4.09 (7) |
2.53 (2) |
|
| Do not know / No response |
6.80 (17) |
9.94 (17) |
0 |
|
| Health insurance regime |
| | | 0.704 |
| Subsidized |
80.80 (202) |
80.70 (138) |
81.01 (64) |
|
| Contributory |
17.60 (44) |
18.13 (31) |
16.46 (13) |
|
| Other |
1.60 (4) |
1.17 (2) |
2.53 (2) |
|
| Personal medical history |
| | | |
| Cardiovascular |
63.60 (159) |
63.74 (109) |
63.29 (50) |
1.000 |
| Metabolic |
28.00 (70) |
25.15 (43) |
34.18 (27) |
0.172 |
| Psychiatric |
38.40 (96) |
47.37 (81) |
18.99 (15) |
<0.001 |
| Degenerative |
35.20 (88) |
42.11 (72) |
20.25 (16) |
0.001 |
| Respiratory |
16.40 (41) |
21.05 (36) |
6.33 (5) |
0.003 |
| Neoplasia-cancer |
4.80 (12) |
6.43 (11) |
1.27 (1) |
0.110 |
| Medications |
| | | |
| Diuretics |
19.20 (48) |
19.88 (34) |
17.72 (14) |
0.687 |
| Tranquilizers |
32.80 (82) |
42.11 (72) |
12.66 (10) |
<0.001 |
| Antiparkinsonian |
6.00 (15) |
7.02 (12) |
3.80 (3) |
0.401 |
| Antidepressants |
27.60 (69) |
36.26 (62) |
8.86 (7) |
<0.001 |
| Antihypertensive |
56.40 (141) |
55.56 (95) |
58.23 (46) |
0.692 |
| Impairment |
| | | |
| Vision impairment |
54.00 (135) |
54.97 (94) |
51.90 (41) |
0.650 |
| Hearing loss |
27.20 (68) |
29.82 (51) |
21.52 (17) |
0.170 |
| Mental |
34.80 (87) |
45.03 (77) |
12.66 (10) |
<0.001 |
| Cognitive |
35.20 (88) |
46.78 (80) |
10.13 (8) |
<0.001 |
| Motor |
36.40 (91) |
46.20 (79) |
15.19 (12) |
<0.001 |
| Multiple |
39.20 (98) |
52.05 (89) |
11.39 (9) |
<0.001 |
| Physical activity |
52.80 (132) |
43.86 (75) |
72.15 (57) |
<0.001 |
| Productive activity |
54.00 (135) |
43.86 (75) |
75.95 (60) |
<0.001 |
P-values: Pearson’s chi-square test and Fisher’s exact test for qualitative variables. Mann-Whitney U test for age.
The medians of the percentiles for the FUMAT-QOLI dimension are shown in Figure 1. The dimensions
with the lowest scores were material well-being, with a median of 16 (IQR: 5–37), followed by
interpersonal relationships, with a median of 37 (IQR: 19–63). Conversely, the highest scores were
observed for the rights dimension, with a median of 84 (IQR: 63–84), and social inclusion, with a
median 75 (IQR: 63–84). Overall, the FUMAT-QOLI showed a median score of 65.5 (IQR: 40–79).
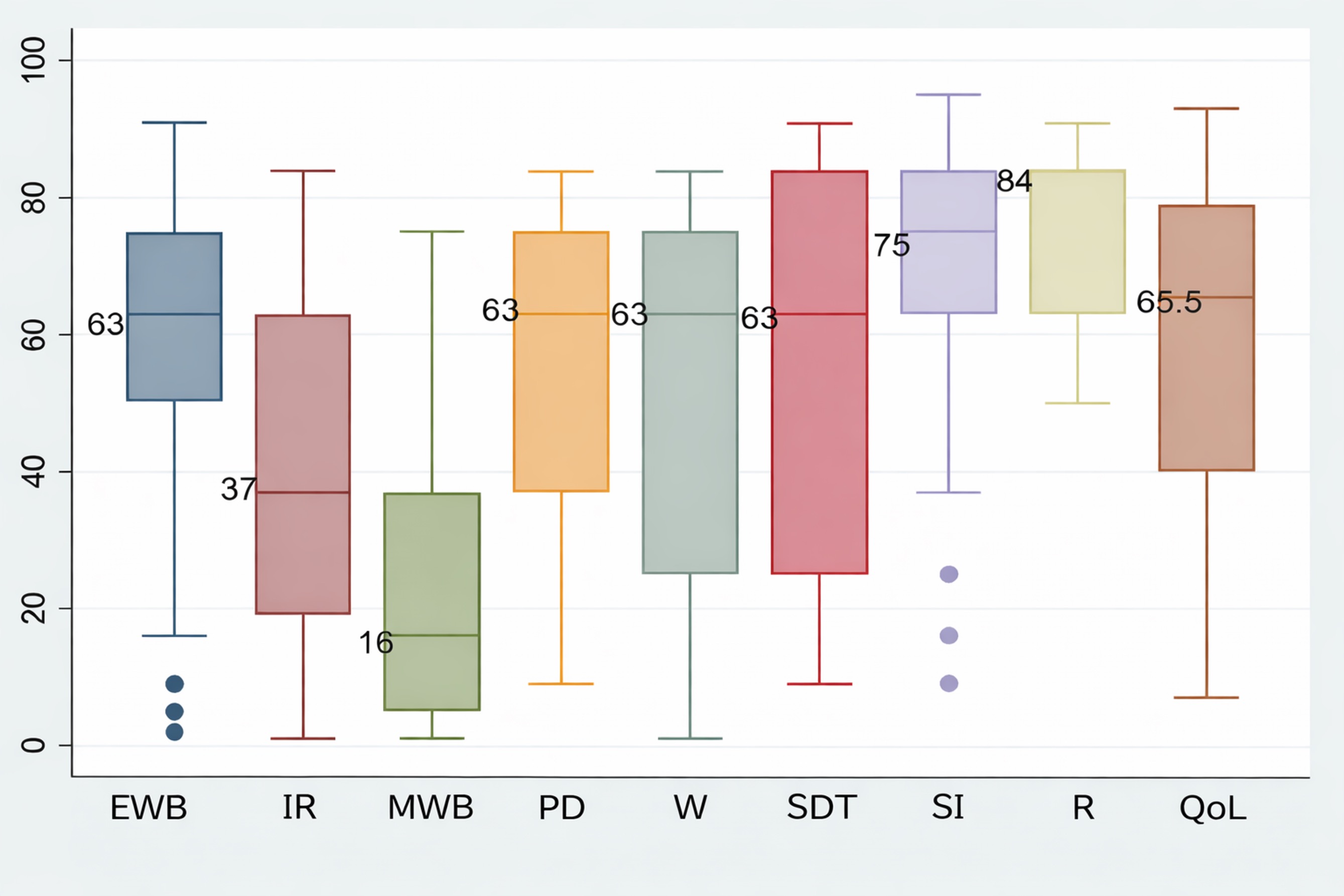
Figure 1. Percentiles of dimensions and the FUMAT quality of life index
EWB: Emotional well-being, IR: Interpersonal relationships, MWB: Material well-being, PD: Personal development, W:
Physical wellbeing, SDT: Self-Determination, SI: Social inclusion, R: Rights, QoL: Quality of life Index.
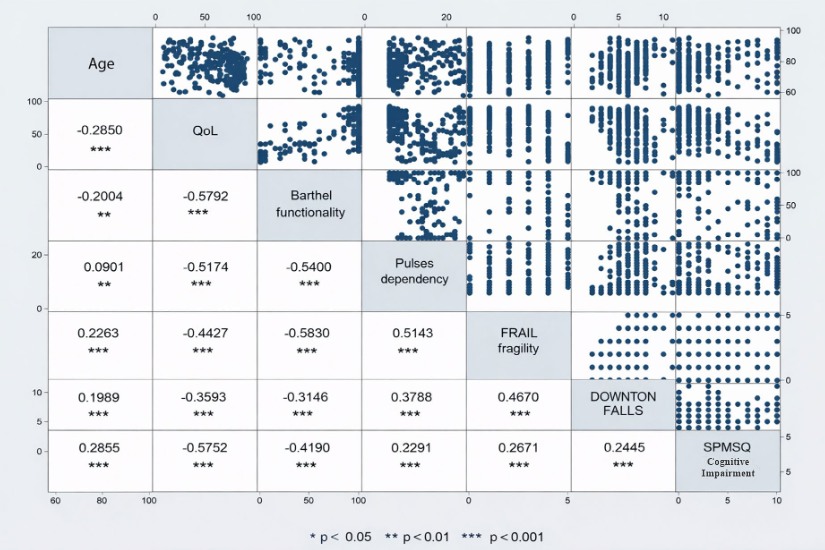
In Spearman’s correlation matrix (Figure 2), age exhibited a negative and statistically significant
correlation with the FUMAT-QOLI (Rho = –0.29, p < 0.001) and with functional independence, as
measured by the Barthel Index (Rho = –0.20, p < 0.01). Although both associations were statistically
significant, their magnitudes corresponded to weak correlations; therefore, while increasing age
tended to be associated with reduced functional independence and quality of life, this relationship
was not strong. No statistically significant correlation was identified between age and the PULSES
profile of dependence.
The strongest correlations were observed between the FUMAT-QOLI and the functional status (Barthel
Index) (Rho = 0.5792, p < 0.001), suggesting a direct association between functional autonomy and a
better perceived well-being. Similarly, a strong negative correlation was found between FUMAT-QOLI
and cognitive impairment (SPMSQ) (Rho = -0.5752, p < 0.001), indicating that cognitive impairment is
associated with lower quality of life.
Likewise, significant associations were observed among frailty (FRAIL scale), dependence (PULSES
profile), and the risk of falls (Downton Index), with positive correlation coefficients among these
measures, indicating their interdependence in the overall functional status of institutionalized older
adults.
Table 2 presents the comparison between tertiles of the FUMAT-QOLI and the categories of functional
status, dependence, frailty, risk of falls, and cognitive impairment. The results indicate statistically
significant associations between the quality-of-life index and the Barthel Index, the PULSES profile,
the FRAIL scale, and the SPMSQ (p < 0.001), whereas no statistically significant differences were
observed for the Downton Fall Risk Index (p = 0.384).
Table 2. Comparison of FUMAT-QOLI tertiles with functional status, dependence, frailty, risk of falls, and cognitive impairment
X
Table 2. Comparison of FUMAT-QOLI tertiles with functional status, dependence, frailty, risk of falls, and cognitive impairment
| Characteristics |
Total % (n)
(250) |
Percentile FUMAT-QOLI |
p-value |
Tertile 1/2
7–76 (171) |
Tertile 3
77–93 (79) |
| Functional status (Barthel Index) |
| | | <0.001 |
| Total dependence |
9.60 (24) |
14.04 (24) |
0 |
|
| Severe dependence |
4.80 (12) |
7.02 (12) |
0 |
|
| Moderate dependence |
6.40 (16) |
9.36 (16) |
0 |
|
| Mild dependence |
14.00 (35) |
15.20 (26) |
11.39 (9) |
|
| Independent |
65.20 (163) |
54.39 (93) |
88.61 (70) |
|
| Dependence (PULSES profile) |
| | | <0.001 |
| Mild impairment |
49.20 (123) |
36.84 (63) |
75.95 (60) |
|
| Moderate impairment or dependence |
15.20 (38) |
16.37 (28) |
12.66 (10) |
|
| Severe impairment or dependence |
35.60 (89) |
46.78 (80) |
11.39 (9) |
|
| Frailty (FRAIL scale) |
| | | <0.001 |
| Not frail |
76.80 (192) |
68.42 (117) |
94.94 (75) |
|
| Frail |
23.20 (58) |
31.58 (54) |
5.06 (4) |
|
| Downton Fall Risk |
| | | 0.384 |
| Moderate risk |
2.40 (6) |
1.75 (3) |
3.80 (3) |
|
| High risk |
97.60 (244) |
98.25 (168) |
96.20 (76) |
|
| Cognitive impairment (SPMSQ) |
| | | <0.001 |
| Normal |
60.00 (150) |
46.20 (79) |
89.87 (71) |
|
| Minimal |
6.00 (15) |
8.19 (14) |
1.27 (1) |
|
| Moderate |
17.20 (43) |
21.64 (37) |
7.59 (6) |
|
| Severe |
16.80 (42) |
23.98 (41) |
1.27 (1) |
|
p-value: Pearson’s chi-square test and Fisher’s exact test.
Regarding functional status, as measured by the Barthel Index, the categories of total, severe, and
moderate dependence were observed exclusively among participants in tertiles 1 and 2. Conversely,
no participants in the third tertile (indicating better quality of life) presented these conditions. In this
latter group, 88.61% were classified as independent, compared with 54.39% in the lower tertiles.
With respect to functional dependence (PULSES profile), the mild impairment category predominated
in the third tertile (75.95%), whereas severe dependence was more prevalent in tertiles 1 and 2
(46.78%), confirming an inverse relationship between dependence and quality of life.
According to the FRAIL scale, 94.94% of participants in the third tertile were classified as not frail,
compared with 68.42% in tertiles 1 and 2. This finding indicates a significant association between
lower frailty and better quality of life.
Although no statistically significant differences were observed in the Downton fall risk index, a
homogeneous high-risk tendency was maintained across all groups.
Finally, according to Pfeiffer’s SPMSQ, 89.87% of participants in the third tertile were classified
as having intact cognitive function, whereas only 46.20% of those in the lower tertiles fell into
this category. Moderate and severe impairment levels were concentrated in tertiles 1 and 2, with
proportions of 21.64% and 23.98%, respectively, reinforcing the influence of cognitive status on the
overall perception of quality of life.
Multivariate analysis showed that participants with cognitive impairment were less likely to be in
the highest tertile of the FUMAT-QOLI scores (OR = 0.34, 95% CI: 0.12; 0.91, p = 0.033), as well as
participants with motor impairment (OR = 0.30, 95% CI: 0.14; 0.64, p = 0.002). When participants
reported engaging in physical activity and productive activities, they showed a greater likelihood
of belonging to the group with the highest scores. While these associations were not statistically
significant, a trend was identified. See Table 3.
Table 3. Multivariate logistic regression model for belonging to the highest tertile of FUMAT-QOLI scores
X
Table 3. Multivariate logistic regression model for belonging to the highest tertile of FUMAT-QOLI scores
| Variables |
OR (95% CI) |
p-value |
| Age |
0.98 (0.94 - 1.01) |
0.345 |
| Respiratory condition |
0.39 (0.13 - 1.18) |
0.099 |
| Impairment |
|
|
| Mental |
0.48 (0.19 - 1.21) |
0.121 |
| Cognitive |
0.34 (0.12 - 0.91) |
0.033 |
| Motor |
0.30 (0.14 - 0.64) |
0.002 |
| Physical activity |
1.70 (0.87 - 3.29) |
0.116 |
| Productive activity |
2.01 (0.98 - 3.86) |
0.054 |
p-value: Wald test.
Discussion
The findings of this study have significant implications for nursing practice in the field of gerontology.
The association between engagement in productive and physical activities and higher scores on the
FUMAT scale underscores the importance of nursing interventions that promote mobility, adapted
exercise, and social integration as essential strategies for preserving and enhancing quality of life in
older adults. Likewise, identifying cognitive and motor disabilities as factors that reduce quality of life
underscores the need for a preventive and early care approach, in which nursing assumes an active
role in detecting functional impairments and designing personalized care plans.
The study identified that participation in productive and physical activities is strongly associated with
higher scores on the FUMAT scale. Similar results were reported in a study conducted in Chile among
older women, which observed significant differences in subjective quality-of-life perceptions between
physically active and inactive individuals, with the former reporting higher levels of satisfaction and
overall well-being following the COVID-19 pandemic
44.
Compared with international studies that have employed the FUMAT scale, the dimension of material
well-being exhibited the lowest scores in this study. This finding aligns with regional evidence from
Paraguay
45,
where a study among 33 residents of peri-urban nursing homes in Asunción reported material well-being
as one of the lowest-scoring dimensions (45 ± 30). These figures underscore the role of social
determinants in quality of life. Studies conducted in Ecuador
22,
Cúcuta, Colombia
46,
and Mexico
47
reported analogous trends, namely, lower ratings of material well-being compared with other
dimensions. By contrast, a study conducted in Spain that employed a short version of the FUMAT scale
(24 items) identified social inclusion, self-determination, and physical well-being as the lowest-scoring
dimensions. These findings suggest that differences in sociocultural context and in the version of the
instrument may modulate the dimensional profiles observed
48.
In this study, the dimensions that obtained the highest scores were rights, social inclusion, and
self-determination, reflecting a positive perception of aspects related to participation, integration,
and personal autonomy. Similar results were observed in a study conducted in Ecuador
22
involving 137 older adults, in which the highest-scoring dimensions were self-determination (63 points)
and personal development and rights (50 points each). Similarly, a study conducted in Spain
24
with a sample of 25 older adults revealed that the highest-scoring dimensions were personal
development (57 points), social inclusion (52 points), and physical well-being (45 points). These
findings confirmed the consistency of these domains as relevant indicators of perceived well-being in
old age.
These results enable the identification of the material well-being dimension of the scale as the
lowest-scoring across the different studies, indicating that it remains a factor limiting the quality of
life of institutionalized older adults. This finding underscores the importance of strengthening public
policies
49
to protect the economic well-being of this population.
The present study demonstrated that cognitive and motor impairments significantly impact quality
of life, consistent with previous research conducted in similar contexts, in which frailty and cognitive
impairment have been identified as determinants of perceived well-being among older adults
50–53.
These findings enrich the body of knowledge in gerontological nursing by providing local evidence that
supports person-centered care practices and encourages professionals to strengthen comprehensive
assessment as a basis for effective interventions. Promoting physical activity, preventing cognitive
and motor impairments, and ensuring social inclusion not only enhance health outcomes but also
reflect nursing’s commitment to the humanization of care for institutionalized older adults.
Another relevant point of comparison emerges from the analysis of the QOLI in relation to mental
health variables. In the present study, psychiatric history and the use of tranquilizers or antidepressants
were found to be associated with lower quality of life. This finding is consistent with other studies
highlighting the negative impact of mental disorders on older adults
54.
However, the present study underscores the need for nursing interventions aimed at promoting mental
health and reducing polypharmacy. These interventions have the potential to enhance the overall
well-being of this population
55.
Among its strengths, the study provides robust empirical evidence through a solid methodological
design based on validated instruments and multivariate analysis. As a result, factors associated with
quality of life were identified with high reliability. Furthermore, the research encompasses a
substantial sample of older adults, thereby enhancing its external validity and enabling the
extrapolation of its findings to similar contexts.
With regard to contributions to nursing practice, education, and research, the study highlights key
elements for strengthening care, such as the need to include person-centered interventions that
promote physical activity and social participation as effective strategies for improving quality of life
in nursing homes
56.
Furthermore, the role of nursing in assessing physical and cognitive functioning is essential for early
detection of impairments that affect quality of life
57.
From the perspective of nursing education, new directions emerge for undergraduate and graduate
nursing curricula, including the comprehensive assessment of older adults, the use of validated scales
in this population, such as the FUMAT scale, and care planning focused on the dimensions of material,
emotional, and social well-being
26.
In this way, nursing professional competence can be strengthened, promoting active aging among
individuals both within and without institutionalization.
Among the limitations to be considered, first, the study was conducted in a single nursing home,
limiting the generalizability of the results to other older adult populations with different
sociodemographic characteristics or living conditions.
Regarding future lines of research, it would be relevant to conduct longitudinal studies to assess
changes in quality of life in this population over time and to identify more accurate predictors.
Examples include a study conducted in Spain that examined the effects of a community-based home
care intervention
58;
research in Peru reporting the impact of a social program among older adults living in extreme
poverty, with the participation of 634 older adults
59;
and studies assessing outcomes in nursing homes involving individuals with cognitive impairment
56.
It is also recommended to expand the research to different types of older people’s homes, including
urban and rural settings
60,
to evaluate potential variations in quality of life according to context, including hospital settings
61.
In view of the above, new lines of research may be considered to evaluate the effects of nursing
interventions on the prevention or limitation of disability and cognitive impairment. In this way, best
care practices can be explored that foster the inclusion and social participation of older adults across
different clinical and community settings, including nursing homes.
Furthermore, it would be relevant to consider validating the 24-item FUMAT scale
62.
Measuring quality of life in individuals with intellectual disabilities or multiple disabilities
63
also remains a challenge, as does examining the effects of various interventions, such as physical
activity plans, dance programs, music therapy
64–67,
and the prevention of polypharmacy
68,
among others that involve the role of gerontological nursing. These efforts would contribute to
continued progress toward excellence in care, promoting humanized care, active aging, and dignified
treatment of older adults.
Conclusions
This study highlights the positive influence of participation in productive activities and physical
activity on the quality of life of older adults and encourages health professionals to prioritize the
prevention of cognitive and motor impairments in this population. Furthermore, this study makes
a significant contribution to the strengthening of gerontological practice by identifying key factors
that impact the quality of life of institutionalized older adults.
Conflict of Interest: The authors declare no conflict of interest.
Funding: This project was funded through a postdoctoral fellowship call 934 from the Ministry of
Science, Technology, and Innovation (Minciencias), Colombia, in partnership with the Albeiro Vargas
and Ángeles Custodios Foundation (FAVAC).
Acknowledgments: The authors acknowledge the multidisciplinary team at the nursing home for
their support in data collection, as well as the older adults who agreed to participate.
References
X
Referencias
DANE. Departamento Administrativo Nacional de Estadística. Colombia registró la tasa de nacimientos más baja de la última década y crecieron las defunciones relacionadas con enfermedades transmitidas por mosquitos. 2024. Consulta: octubre 07, 2025. Disponible en: https://www.dane.gov.co/files/operaciones/EEVV/cp-EEVV-Itrim2024.pdf
X
Referencias
Venegas-Sanabria C, Cavero-Redondo I, Martínez-Vizcaíno V, Cano-Gutiérrez A, Álvarez-Bueno C. Effect of multicomponent exercise in cognitive impairment: a systematic review and meta-analysis. BMC Geriatrics. 2022;22:617. https://doi.org/10.1186/s12877-022-03302-1
X
Referencias
Organización de las Naciones Unidas. Mirada global. Historias humanas. Las enfermedades no transmisibles causan el 75 % de las muertes globales y van en aumento. 2023. Consulta: octubre 07, 2025. Disponible en: https://news.un.org/es/story/2023/05/1521192
X
Referencias
Baixinho CL, Madeira C, Alves S, Henriques MA, Dixe M. Falls and Preventive Practices among Institutionalized Older People. Int J Environ Res Public Health. 2022;19. https://doi.org/10.3390/ijerph19137577
X
Referencias
Manrique-Anaya Y, Pérez J, Sigalat E, Torres C. Apoyo social, capacidad funcional y calidad de vida en adultos mayores de centros de bienestar. Enfermería Global. 2025;76:1–15. https://doi.org/10.6018/eglobal.636591
X
Referencias
Lozano-Vidal R, López-Pisa RM, Boyero-Granados A, Recio-Ramos S, Padín-Minaya C, Garzón-Quiñónez M, et al. Estratificación de la población mayor de 65 años en grupos de riesgo clínico: características y valoración enfermera. Enfermería Clínica. 2014;24(5):290–5. http://dx.doi.org/10.1016/j.enfcli.2014.06.001
X
Referencias
García-Walker V. Elder’s life course theory and person-centered research: A lens for conducting ethical nursing research and mental health nursing practice with older adults aging with the diagnosis of schizophrenia. J Psychiatr Ment Health Nurs. 2022. https://doi.org/10.1111/jpm.12819
X
Referencias
Briceño-Martínez A, Contreras-Pava A, León-Cely N, Araque-Peñaloza D, Rivera-Porras D. Caracterización de la calidad de vida en adultos mayores pertenecientes a cuatro asociaciones de Cúcuta mediante la Escala FUMAT. Rev Cient Signos Fónicos. 2021;7(2):1–25. https://ojs.unipamplona.edu.co/index.php/cdh/article/view/1297
X
Referencias
Rodríguez-Jiménez M, Pérez-Jorge D, Puerta-Araña I, Ariño-Mateo E. Quality of Life in Deafblind People and Its Effect on the Processes of Educational Adaptation and Social Inclusion in Canary Islands, Spain. Education Sciences. 2022;12:490. https://doi.org/10.3390/educsci12070490
X
Referencias
Duarte-Ayala RE, Velasco-Rojano A. Validación psicométrica del índice de Barthel en adultos mayores mexicanos. Horizonte Sanitario. 2022;21(1). https://doi.org/10.19136/hs.a21n1.4519
X
Referencias
Martínez-Hernández B, Rosas-Carrasco O, López-Teros M, González-Rocha A, Muñoz-Aguirre P, Palazuelos-González R, et al. Association between physical activity and physical and functional performance in non-institutionalized Mexican older adults: a cohort study. BMC Geriatrics. 2022;22:1–11. https://doi.org/10.1186/s12877-022-03083-7
X
Referencias
Dos-Santos V, Bassi-Dibai D, Ribeiro C, Nunes D, Marinho S, De-Oliveira G, et al. Barthel Index is a valid and reliable tool to measure the functional independence of cancer patients in palliative care. BMC Palliative Care. 2022;21:1–7. https://doi.org/10.1186/s12904-022-01017-z
X
Referencias
Cantillo-Medina C, Ramírez-Perdomo C, Perdomo-Romero A. Habilidad de cuidado en cuidadores familiares de personas con enfermedad crónica y sobrecarga percibida. Ciencia y Enfermería. 2018;24(16):1–12. http://dx.doi.org/10.4067/s0717-95532018000100216
X
Referencias
Parra MD, Torres CC, Arboleda LB, Rivera R, Franco S, Santos J. Effectiveness of an educational nursing intervention on caring ability and burden in family caregivers of patients with chronic non-communicable diseases: A preventive randomized controlled clinical trial. Investigación y Educación en Enfermería. 2019;37(1). http://dx.doi.org/10.17533/udea.iee.v37n1e04
X
Referencias
Parada D, Carreño-Moreno S, Chaparro-Díaz L. Soledad, ansiedad y depresión en la adopción del rol de cuidador familiar del paciente crónico. Revista Cuidarte. 2023;14(1):e2451. http://dx.doi.org/10.15649/cuidarte.2451
X
Referencias
Arboleda V, Muñoz-Rodríguez D, Segura A, Robledo C, Cardona D, et al. Profile in frail older people over 60 years of age in five Colombian cities, 2021. Medicina UPB. 2025;44(1). http://dx.doi.org/10.18566/medupb.v44n1.a03
X
Referencias
Rosas-Carrasco O, Cruz-Arenas E, Parra-Rodríguez L, García-González AI, Contreras-González LH, Szlejf C. Cross-cultural adaptation and validation of the FRAIL Scale to assess frailty in Mexican adults. Journal of the American Medical Directors Association. 2016;17(12):1094–8. http://dx.doi.org/10.1016/j.jamda.2016.07.008
X
Referencias
Mateo-Cervera A, Fernández-Carrasco S. Revisión de la validez de las escalas de valoración del riesgo de caídas en pacientes hospitalizados. Rev Esp Geriatr Gerontol. 2023;1(3):1–8. https://doi.org/10.1016/j.regg.2022.03.005
X
Referencias
Del Brutto OH, Mera RM, Rumbea DA, Recalde BY, Sedler MJ. Testing the reliability of the Downton Fall Risk Index for predicting incident falls in community-dwelling older adults. Rev Ecuatoriana de Neurología. 2022;31(3). http://dx.doi.org/10.46997/revecuatneurol31300016
X
Referencias
Gutiérrez-Valencia M, Leache L, Saiz LC. Review of the validity of fall risk assessment scales in hospitalised patients. Rev Esp Geriatr Gerontol. 2022;57(3):1–5. https://doi.org/10.1016/j.regg.2022.03.005
X
Referencias
Sanchis J, Bonanad C, García-Blas S, Ruiz V, Fernández-Cisnal A, Sastre C, et al. Long-term prognostic value of cognitive impairment on top of frailty in older adults after acute coronary syndrome. Journal of Clinical Medicine. 2021;10(3). https://doi.org/10.3390/jcm10030444
X
Referencias
Angamarca D, Muñoz D, González A, Domínguez J. Eficacia del Mini Mental y Pfeiffer (SPMSQ) para detectar deterioro cognitivo en mayores de 65 años. Revista Investigación en Salud. 2020;3(9):149–57. https://doi.org/10.33996/revistavive.v3i9.55
X
Referencias
Mamani R, Roque E, Colque N, Solorzano M. Actividad física y el deterioro cognitivo en adultos mayores. Revista Ciencias de la Actividad Física. 2023;24(1):1–14. https://doi.org/10.29035/rcaf.24.1.8
X
Referencias
Castillo MA, Hernández J. Percepción subjetiva de la calidad de vida según niveles de actividad física en mujeres mayores chilenas tras la pandemia de COVID-19. Retos. 2025;63:868–77. https://doi.org/10.47197/retos.v63.108693
X
Referencias
Briceño-Martínez A, Contreras-Pava P, León-Cely N, Araque-Peñaloza D, Rivera-Porras D. Caracterización de la calidad de vida en adultos mayores pertenecientes a cuatro asociaciones de Cúcuta mediante la Escala FUMAT. Rev Cient Signos Fónicos. 2021;29. https://ojs.unipamplona.edu.co/index.php/cdh/es/article/view/1297
X
Referencias
Rodríguez-Rodríguez V, Rojo-Pérez F, Pérez C, Molina-Martínez M, Fernández-Mayoralas G, Sánchez-González D, et al. The Impact of COVID-19 on Nursing Homes: Study Design and Population Description. Int J Environ Res Public Health. 2022;19:16629. https://doi.org/10.3390/ijerph192416629
X
Referencias
Ghența M, Matei A, Rothe F, Aartsen M, Precupetu I. Assessing the transferability potential of policy practices for older people. Archives of Public Health. 2025;83(56):1–9. https://doi.org/10.1186/s13690-025-01548-w
X
Referencias
Albuquerque G, Faleiros F, Corbo L, Maia E, França I, Bezerra S, et al. Validation of nursing educational technology for neurogenic bowel rehabilitation in people with spinal cord injury. Revista Cuidarte. 2024;15(2). https://doi.org/10.15649/cuidarte.3705
X
Referencias
Hu W, Chu J, Zhu Y, Chen X, Sun N, Han Q, et al. The longitudinal association between frailty, cognition, and quality of life in older Europeans. Gerontological Society of America. 2023;78(5):809–18. https://doi.org/10.1093/geronb/gbad013
X
Referencias
Martins R, Gomes S, Vicente P, Carvalho N, Batista S. The quality of life of people with multiple sclerosis in Portugal. Revista Cuidarte. 2024;15(2). https://doi.org/10.15649/cuidarte.2841
X
Referencias
Lee SL, Pearce E, Ajnakina O, Johnson S, Lewis G, Mann F, et al. The association between loneliness and depressive symptoms among adults aged 50 years and older: a 12-year population-based cohort study. The Lancet Psychiatry. 2021;8(1):48–57. http://dx.doi.org/10.1016/S2215-0366(20)30383-7
X
Referencias
Wang H-I, Gilbody S, Littlewood E, Baird K, Ekers D, McMillan D, et al. Cost-utility of behavioural activation for mitigating psychological impacts of COVID-19 on socially isolated older adults with depression and multiple long-term conditions compared with usual care. BMJ Mental Health. 2025;28:1–9. http://dx.doi.org/10.1136/bmjment-2024-301270
X
Referencias
Díaz-Veiga P, Sancho M, García Á, Rivas E, Abad E, Suárez N, et al. Efectos del Modelo de Atención Centrado en la Persona en la calidad de vida de personas con deterioro cognitivo de centros gerontológicos. Rev Esp Geriatr Gerontol. 2014;49(6):266–71. http://dx.doi.org/10.1016/j.regg.2014.06.003
X
Referencias
Khodadad-Kashi S, Sadat-Mirzazadeh Z, Saatchian V. Systematic Review and Meta-Analysis of Resistance Training on Quality of Life, Depression, Muscle Strength, and Functional Exercise Capacity in Older Adults Aged 60 Years or More. Biological Research for Nursing. 2022;25(1):1–22. https://doi.org/10.1177/10998004221120945
X
Referencias
Palacios-Navarro G, Santamaría R, Ramos P. Effects of a home care community-dwelling intervention on cognition, mental health, loneliness and quality of life in elder people: The VERA study. Int J Med Inform. 2024;185:e105378. https://doi.org/10.1016/j.ijmedinf.2024.105378
X
Referencias
Tavares D, Bolina A, Dias F, Ferreira P, Haas V. Quality of life of elderly: comparison between urban and rural areas. Invest Educ Enferm. 2013;31(3):401–13. https://doi.org/10.17533/udea.iee.20701
X
Referencias
Porras-Jiménez Y, Álvarez-Nieto C, Romero-Granados K, Pinzón-Ordoñez C, López-Medina I. Effectiveness of laughter therapy with healthcare clowns on the mood of hospitalised adults. Revista Cuidarte. 2025;16(1). https://doi.org/10.15649/cuidarte.4375
X
Referencias
Cárdenas P, Rodríguez-Blázquez C, João M, Ayala A, Rojo-Pérez F, Fernández-Mayoralas G, et al. Validation of the Spanish Version of the Fear of COVID-19 Scale (FCV-19S) in Long-Term Care Settings. Int J Environ Res Public Health. 2022;19:16183. https://doi.org/10.3390/ijerph192316183
X
Referencias
Verdugo MA, Gómez LE, Schalock RL, Arias B, Navas P. Measuring quality of life in people with intellectual and multiple disabilities: Validation of the San Martín scale. Research in Developmental Disabilities. 2014;35:75–86. https://doi.org/10.1016/j.ridd.2013.10.025
X
Referencias
Gonnord T, Clarys D, Boucard G, Esnard C. Positive impact of social relationships fostered by physical and/or cognitive group activity on older people’s quality of life: PRISMA systematic review. Frontiers in Psychology. 2023;14:e1166072. http://dx.doi.org/10.3389/fpsyg.2023.1166072
X
Referencias
Mohammadi Z, Mirzaei T, Ravari A, Kamiab Z. Comparison the effect of Otago and chair squat exercises on the fear of falling and the quality of life of the older adults: a clinical trial study. Aging Clin Exp Res. 2025;37(66):1–9. https://doi.org/10.1007/s40520-025-02951-7
X
Referencias
Maissan MJE, Van Raaij BFM, Festen J, Gussekloo J. A qualitative study regarding older people’s goals of care in relation to frailty status: finding meaning in ‘smaller things’ in life. Age and Ageing. 2025;54(afaf022):1–11. https://doi.org/10.1093/ageing/afaf022
X
Referencias
Jandaghian-Bidgoli M, Jamalnia S, Pashmforosh M, Shaterian N, Darabiyan P, Rafi A. The effect of Orem self-care model on the improvement of symptoms and quality of life in patients with diabetes: a scoping review. Investigación y Educación en Enfermería. 2023;42(1):e08. https://doi.org/10.17533/udea.iee.v42n1e08
X
Referencias
Andrews N, Brooks C, Board M, Fraser S, Latter S, Aplin K. Medicine Optimisation and Deprescribing Intervention Outcomes for Older People with Dementia or Mild Cognitive Impairment: A Systematic Review. Drugs & Aging. 2025. https://doi.org/10.1007/s40266-025-01189-2
Organización Mundial de la Salud. Reunión de Ministros de Salud del G7 en Kobe: alcanzar la cobertura sanitaria universal centrándose en el envejecimiento saludable y activo [Internet]. 2016. p. 2–3. Consulta: enero 09, 2025. https://www.who.int/es/director-general/speeches/detail/g7-kobe-health-ministers-meeting-attaining-universal-health-coverage-focusing-on-healthy-and-active-ageing
DANE. Departamento Administrativo Nacional de Estadística. Colombia registró la tasa de nacimientos más baja de la última década y crecieron las defunciones relacionadas con enfermedades transmitidas por mosquitos. 2024. Consulta: octubre 07, 2025. https://www.dane.gov.co/files/operaciones/EEVV/cp-EEVV-Itrim2024.pdf
World Health Organization. Ageing and health. 2025. p. 6–9. Consulta: octubre 07, 2025. https://www.who.int/news-room/fact-sheets/detail/ageing-and-health
Stephany T. Nursing and aging. Am J Nurs. 2019;119(10):10. https://doi.org/10.1097/01.NAJ.0000586068.10122.43
García L, Quevedo M, La Rosa Y, Leyva A. Calidad de vida percibida por adultos mayores. Revista Electrónica Medinay. 2020;27(1):16–25. https://www.medigraphic.com/pdfs/revciemedhab/cmh-2020/cmh201c.pdf
Gómez L, Verdugo M, Arias B, Navas P. Evaluación de la calidad de vida en personas mayores y con discapacidad: la Escala FUMAT. Interv Psicosoc. 2008;17:189–99. https://journals.copmadrid.org/pi/art/5938b4d054136e5d59ada6ec9c295d7a
Ministerio de Salud y Protección Social de Colombia. Decreto 681 de 2022. Política Pública Nacional de Envejecimiento y Vejez 2022–2031. 2022. https://www.minsalud.gov.co/Normatividad_Nuevo/Decreto%20No.%20681%20de%202022.pdf
Venegas-Sanabria C, Cavero-Redondo I, Martínez-Vizcaino V, Cano-Gutierrez A, Álvarez-Bueno C. Effect of multicomponent exercise in cognitive impairment: a systematic review and meta-analysis. BMC Geriatr. 2022;22(617). https://doi.org/10.1186/s12877-022-03302-1
Organización de las Naciones Unidas. Las enfermedades no transmisibles causan el 75 % de las muertes globales y van en aumento. 2023. https://news.un.org/es/story/2023/05/1521192
Baixinho CL, Madeira C, Alves S, Henriques MA, Dixe M. Falls and Preventive Practices among Institutionalized Older People. Int J Environ Res Public Health. 2022;19. https://doi.org/10.3390/ijerph19137577
Fuentes N, Lomelí R, Colmenares V. Calidad de vida del adulto mayor: una oportunidad para construir procesos de intervención desde el trabajo social. Políticas Soc Sect. 2024;2(3):121–39. https://politicassociales.uanl.mx/index.php/pss/article/view/111/91
Ministerio de Salud y Protección Social de Colombia. Minsalud actualiza política de envejecimiento y vejez. 2021. https://www.minsalud.gov.co/Paginas/Minsalud-actualiza-politica-de-envejecimiento-y-vejez.aspx
Manrique-Anaya Y, Pérez J, Sigalat E, Torres C. Apoyo social, capacidad funcional y calidad de vida en adultos mayores de centros de bienestar. Enfermería Global. 2025;76:1–15. https://doi.org/10.6018/eglobal.636591
Varela L. Health and quality of life in the elderly. Rev Perú Med Exp Salud Publica. 2016;33(2):199–201. http://dx.doi.org/10.17843/rpmesp.2016.332.2196
Martínez O, Mamarero O, González CLM. Calidad de vida del adulto mayor en un consultorio médico del municipio Jaruco. Rev Ciencias Médicas La Habana. 2016;22(1):30–41. https://revcmhabana.sld.cu/index.php/rcmh/article/view/925
Dogra S, Dunstan DW, Sugiyama T, Stathi A, Gardiner PA, Owen N. Active Aging and Public Health: Evidence, Implications, and Opportunities. Annu Rev Public Health. 2022;43:439–59. https://doi.org/10.1146/annurev-publhealth-052620-091107
Lozano-Vidal R, López-Pisa RM, Boyero-Granados A, Recio-Ramos S, Padín-Minaya C, Garzón-Quiñonez M, et al. Estratificación de la población mayor de 65 años en grupos de riesgo clínico. Enfermería Clínica. 2014;24(5):290–5. http://dx.doi.org/10.1016/j.enfcli.2014.06.001
García-Walker V. Elder’s life course theory and person-centered research: A lens for conducting ethical nursing research and mental health nursing practice with older adults aging with the diagnosis of schizophrenia. Psychiatr Ment Heal Nurs. 2022;1–17. https://doi.org/10.1111/jpm.12819
Briceño-Martinez A, Contreras-Pava A, León-Cely N, Araque-Peñaloza D, Rivera-Porras D. Caracterización de la calidad de vida en adultos mayores pertenecientes a cuatro asociaciones de Cúcuta mediante la Escala FUMAT. Rev Cient Signos Fónicos. 2021;7(2):1–25. https://ojs.unipamplona.edu.co/index.php/cdh/article/view/1297
Astorquiza B, Chingal O. ¿Cómo están nuestros ancianos? Una exploración empírica de la calidad de vida de las personas mayores en Colombia. Rev la CEPAL. 2019;(129):139–61. https://repositorio.cepal.org/server/api/core/bitstreams/d11de9d6-e529-4453-ab0d-410d002d5efd/content
López M, Aguilar L, MJ M. La calidad de vida percibida por personas adultas mayores urbanas no institucionalizadas en Tuxtla Gutiérrez, Chiapas. An en Gerontol. 2022;14(1):73–95. https://revistas.ucr.ac.cr/index.php/gerontologia/article/view/5012
Palma E, Peña A, Quinde V. FUMAT: Evaluación de la calidad de vida de los adultos mayores pospandemia. Rev Cient Arbitr Multidiscip PENTACIENCIAS. 2022;4(6):507–19. https://editorialalema.org/index.php/pentaciencias/article/view/400
Villalba A, Ramos S. Condiciones de vida y bienestar en la vejez: análisis de adultos mayores del Hospital Distrital de Ñemby, Paraguay. Scienti Americana. 2025;12(1):14–8. https://dx.doi.org/10.30545/scientiamericana.2025.ene-abr.3
Rodriguez-Jimenez M, Perez-Jorge D, Puerta-Araña I, Ariño-Mateo E. Quality of Life in Deafblind People and Its Effect on the Processes of Educational Adaptation and Social Inclusion in Canary Islands, Spain. Educ Sci. 2022;12:490. https://doi.org/10.3390/educsci12070490
Morales S, Calvo M. Deterioro cognitivo y calidad de vida en el adulto mayor del Centro de Jubilados Naciones Unidas del Instituto Ecuatoriano de Seguridad Social IESS de la ciudad de Quito, año 2020. Universidad Tecnológica Indoamérica; 2020. https://repositorio.uti.edu.ec/items/5dc50868-933c-4da3-9473-4947c1ffab15
Verdugo M, Gómez L, Arias B. Evaluación de la calidad de vida en personas mayores. La Escala FUMAT. Instituto Universitario de Integración en la Comunidad. Salamanca; 2009. http://sid.usal.es/idocs/F8/FDO23248/herramientas_4.pdf
Duarte-Ayala RE, Velasco-Rojano A. Validación psicométrica del índice de Barthel en adultos mayores mexicanos. Horiz Sanit. 2022;21(1). https://doi.org/10.19136/hs.a21n1.4519
Martinez-Hernandez B, Rosas-Carrasco O, Lopez-Teros M, Gonzalez-Rocha A, Muñoz-Aguirre P, Palazuelos-Gonzalez R, et al. Association between physical activity and physical and functional performance in non-institutionalized Mexican older adults: a cohort study. BMC Geriatr. 2022;22:1–11. https://doi.org/10.1186/s12877-022-03083-7
Dos-Santos V, Bassi-Dibai D, Ribeiro C, Nunes D, Marinho S, De-Oliveira G, et al. Barthel Index is a valid and reliable tool to measure the functional independence of cancer patients in palliative care. BMC Palliat Care. 2022;21:1–7. https://doi.org/10.1186/s12904-022-01017-z
Cantillo-Medina C, Ramírez-Perdomo C, Perdomo-Romero A. Habilidad de cuidado en cuidadores familiares de personas con enfermedad crónica y sobrecarga percibida. Cienc y Enfermería. 2018;24(16):1–12. http://dx.doi.org/10.4067/s0717-95532018000100216
Parra MD, Torres CC, Arboleda LB, Rivera R, Franco S, Santos J. Effectiveness of an Educational Nursing Intervention on Caring Ability and Burden in Family Caregivers of Patients with Chronic Non-Communicable Diseases: A Preventive Randomized Controlled Clinical Trial. Investig y Educ Enferm. 2019;37(1). http://dx.doi.org/10.17533/udea.iee.v37n1e04
Parada D, Carreño-Moreno S, Chaparro-Diaz L. Soledad, ansiedad y depresión en la adopción del rol de cuidador familiar del paciente crónico. Rev Cuid. 2023;14(1):e2451. http://dx.doi.org/10.15649/cuidarte.2451
Davis-Varona L. Evaluación del estado de fragilidad en adultos mayores aplicando la escala FRAIL. Arch méd Camagüey. 2024;28:e10046. https://revistaamc.sld.cu/index.php/amc/article/view/10046
Arboleda V, Muñoz-Rodríguez D, Segura A, Robledo C, Cardona D, et al. Profile in frail older people over 60 years of age in five Colombian cities, 2021. Med UPB. 2025;44(1). http://dx.doi.org/10.18566/medupb.v44n1.a03
Rosas-Carrasco O, Cruz-Arenas E, Parra-Rodríguez L, García-González AI, Contreras-González LH, Szlejf C. Cross-Cultural Adaptation and Validation of the FRAIL Scale to Assess Frailty in Mexican Adults. J Am Med Dir Assoc. 2016;17(12):1094–8. http://dx.doi.org/10.1016/j.jamda.2016.07.008
Mateo-Cervera A, Fernández-Carrasco S. Revisión de la validez de las escalas de valoración del riesgo de caídas en pacientes hospitalizados. Rev Esp Geriatr Gerontol. 2023;1(3):1–8. https://doi.org/10.1016/j.regg.2022.03.005
Del Brutto OH, Mera RM, Rumbea DA, Recalde BY, Sedler MJ. Testing the reliability of the Downton Fall Risk Index for predicting incident falls in community-dwelling older adults: A prospective study. Rev Ecuat Neurol. 2022;31(3). http://dx.doi.org/10.46997/revecuatneurol31300016
Gutiérrez-Valencia M, Leache L, Saiz LC. Revisión de la validez de las escalas de valoración del riesgo de caídas en pacientes hospitalizados. Rev Esp Geriatr Gerontol. 2022;57(3):1–5. https://doi.org/10.1016/j.regg.2022.03.005
Sanchis J, Bonanad C, García-Blas S, Ruiz V, Fernández-Cisnal A, Sastre C, et al. Long-Term Prognostic Value of Cognitive Impairment on Top of Frailty in Older Adults after Acute Coronary Syndrome. J Clin Med. 2021;10(3). https://doi.org/10.3390/jcm10030444
Angamarca D, Muñoz D, González A, Domínguez J. Eficacia del Mini Mental y Pfeiffer (SPMSQ) para detectar deterioro cognitivo en mayores de 65 años. Rev Investig en Salud. 2020;3(9):149–57. https://doi.org/10.33996/revistavive.v3i9.55
Mamani R, Roque E, Colque N, Solórzano M. Actividad física y el deterioro cognitivo en adultos mayores. Rev Cienc Act Fís. 2023;24(1):1–14. https://doi.org/10.29035/rcaf.24.1.8
Hosmer D, Lemeshow S. Model-Building Strategies and Methods for Logistic Regression. In: Applied Logistic Regression. 2013. p. 89–150. https://mybiostats.wordpress.com/wp-content/uploads/2015/03/model_building_strategies_and_methods_for_logistic_regression.pdf
Torres C, Vargas A. Perfil salud y calidad de vida de personas mayores de un Centro Gerontológico de Bucaramanga. Mendeley Data. 2025. https://doi.org/10.17632/6c4pt8zfgb.1
Castillo MA, Hernández J. Percepción subjetiva de la calidad de vida según niveles de actividad física en mujeres mayores chilenas tras la pandemia de COVID-19. Retos. 2025;63:868–77. https://doi.org/10.47197/retos.v63.108693
Meza J, Insaurralde A, Alviso D. Modelo matemático para estimar el índice de calidad de vida en adultos mayores usando la encuesta FUMAT. Mem Inst Investig Cienc Salud. 2021;19(3):44–53. http://dx.doi.org/10.18004/mem.iics/1812-9528/2021.019.03.44
Briceño-Martínez A, Contreras-Pava P, León-Cely N, Araque-Peñaloza D, Rivera-Porras D. Caracterización de la calidad de vida en adultos mayores pertenecientes a cuatro asociaciones de Cúcuta mediante la Escala FUMAT. Rev Cient Signos Fónicos. 2021;29. https://ojs.unipamplona.edu.co/index.php/cdh/es/article/view/1297
Maya E, Hernández J, Vargas X, Guzmán E. Evaluación de la calidad de vida de adultos mayores no institucionalizados de la CDMX a través de la escala FUMAT. Eureka. 2018;15(1):65–77. https://docs.bvsalud.org/biblioref/2018/06/885117/eureka-15-1-12.pdf
Rodríguez-Rodríguez V, Rojo-Pérez F, Pérez C, Molina-Martínez M, Fernández-Mayoralas G, Sánchez-González D, et al. The Impact of COVID-19 on Nursing Homes: Study Design and Population Description. Int J Environ Res Public Health. 2022;19:16629. https://doi.org/10.3390/ijerph192416629
Ghența M, Matei A, Rothe F, Aartsen M, Precupetu I. Assessing the transferability potential of policy practices for older people. Arch Public Health. 2025;83(56):1–9. https://doi.org/10.1186/s13690-025-01548-w
Albuquerque G, Faleiros F, Corbo L, Maia E, França I, Bezerra S, et al. Validation of nursing educational technology for neurogenic bowel rehabilitation in people with spinal cord injury. Rev Cuid. 2024;15(2). https://doi.org/10.15649/cuidarte.3705
Hu W, Chu J, Zhu Y, Chen X, Sun N, Han Q, et al. The Longitudinal Association Between Frailty, Cognition, and Quality of Life in Older Europeans. Gerontol Soc Am. 2023;78(5):809–18. https://doi.org/10.1093/geronb/gbad013
Pavel A, Paun R, Matei V, Rosca A, Tudose C. Quality of Life in People With Subjective Cognitive Decline. Alpha Psychiatry. 2023;24(2):60–4. http://dx.doi.org/10.5152/alphapsychiatry.2023.221007
Martins R, Gomes S, Vicente P, Carvalho N, Batista S. The quality of life of people with multiple sclerosis in Portugal. Rev Cuid. 2024;15(2). https://doi.org/10.15649/cuidarte.2841
Lee SL, Pearce E, Ajnakina O, Johnson S, Lewis G, Mann F, et al. The association between loneliness and depressive symptoms among adults aged 50 years and older: a 12-year population-based cohort study. The Lancet Psychiatry. 2021;8(1):48–57. http://dx.doi.org/10.1016/S2215-0366(20)30383-7
Wang H-I, Gilbody S, Littlewood E, Baird K, Ekers D, McMillan D, et al. Cost-utility of behavioural activation for mitigating psychological impacts of COVID-19 on socially isolated older adults with depression and multiple long-term conditions compared with usual care: results from a pragmatic randomised controlled trial. BMJ Ment Health. 2025;28:1–9. http://dx.doi.org/10.1136/bmjment-2024-301270
Díaz-Veiga P, Sancho M, García Á, Rivas E, Abad E, Suárez N, et al. Efectos del Modelo de Atención Centrado en la Persona en la calidad de vida de personas con deterioro cognitivo de centros gerontológicos. Rev Esp Geriatr Gerontol. 2014;49(6):266–71. http://dx.doi.org/10.1016/j.regg.2014.06.003
Khodadad-Kashi S, Sadat-Mirzazadeh Z, Saatchian V. Systematic Review and Meta-Analysis of Resistance Training on Quality of Life, Depression, Muscle Strength, and Functional Exercise Capacity in Older Adults Aged 60 Years or More. Biol Res Nurs. 2022;25(1):1–22. https://doi.org/10.1177/10998004221120945
Palacios-Navarro G, Santamaría R, Ramos P. Effects of a home care community-dwelling intervention on cognition, mental health, loneliness and quality of life in elder people: The VERA study. Int J Med Inform. 2024;185:e105378. https://doi.org/10.1016/j.ijmedinf.2024.105378
Chui H, Valdivia M. Los programas sociales y la calidad de vida de las personas adultas mayores en situación de extrema pobreza. O Mundo da Saúde. 2024;48:e15962024. https://doi.org/10.15343/0104-7809.202448e15962024E
Taveres D, Bolina A, Dias F, Ferreira P, Hass V. Quality of life of elderly: Comparison between urban and rural areas. Invest Educ Enferm. 2013;31(3):401–13. https://doi.org/10.17533/udea.iee.20701
Porras-Jimenez Y, Alvarez-Nieto C, Romero-Granados K, Pinzón-Ordoñez C, López-Medina I. Effectiveness of laughter therapy with healthcare clowns on the mood of hospitalised adults. Rev Cuid. 2025;16(1). https://doi.org/10.15649/cuidarte.4375
Cárdenas P, Rodríguez-Blázquez C, João M, Ayala A, Rojo-Pérez F, Fernández-Mayoralas G, et al. Validation of the Spanish Version of the Fear of COVID-19 Scale (FCV-19S) in Long-Term Care Settings. Int J Environ Res Public Health. 2022;19:16183. https://doi.org/10.3390/ijerph192316183
Verdugo MA, Go LE, Schalock RL, Arias B, Navas P. Measuring quality of life in people with intellectual and multiple disabilities: Validation of the San Martín scale. Res Dev Disabil. 2014;35:75–86. https://doi.org/10.1016/j.ridd.2013.10.025
Gonnord T, Clarys D, Boucard G, Esnard C. Positive impact of social relationships fostered by physical and/or cognitive group activity on older people’s quality of life: PRISMA systematic review. Front Psychol. 2023;14:e1166072. http://dx.doi.org/10.3389/fpsyg.2023.1166072
Mohammadi Z, Mirzaei T, Ravari A, Kamiab Z. Comparison the effect of Otago and chair squat exercises on the fear of falling and the quality of life of the older adults: a clinical trial study. Aging Clin Exp Res. 2025;37(66):1–9. https://doi.org/10.1007/s40520-025-02951-7
Maissan MJE, Van Raaij BFM, Festen J, Gussekloo J. A qualitative study regarding older people’s goals of care in relation to frailty status: finding meaning in “smaller things” in life. Age Ageing. 2025;54:afaf022. https://doi.org/10.1093/ageing/afaf022
Jandaghian-Bidgoli M, Jamalnia S, Pashmforosh M, Shaterian N, Darabiyan P, Rafi A. The effect of Orem self-care model on the improvement of symptoms and quality of life in patients with diabetes: A scoping review. Investig y Educ Enferm. 2023;42(1):e08. https://doi.org/10.17533/udea.iee.v42n1e08
Andrews N, Brooks C, Board M, Fraser S, Latter S, Aplin K. Medicine Optimisation and Deprescribing Intervention Outcomes for Older People with Dementia or Mild Cognitive Impairment: A Systematic Review. Drugs Aging. 2025. https://doi.org/10.1007/s40266-025-01189-2