Rev Cuid. 2025; 16(3): e4255
Abstract
Introduction: In recent years, the workload of nursing professionals in intensive care units (ICUs) has been described. Identifying associated factors may contribute to improving nursing care planning.
Objective: To determine predictors associated with nursing workload in ICU settings using a sample of records collected before and during the first peak of the COVID-19 pandemic.
Materials and Methods: This was an analytical cross-sectional study. A total of 97 ICU patient records were included. Descriptive and multivariate analyses were performed using robust linear regression, with the primary outcome being workload measured with the Nursing Activities Score (NAS).
Results: The mean age was 57.67 ± 17.78 years, and 68.04% (n=66) were men. Statistically significant differences were observed between the pre-pandemic period and the first peak of the pandemic for variables such as disease category, ICU type, Sequential Organ Failure Assessment (SOFA) score, and number of nurses (p<0.001). A difference in median NAS values was observed, with 60.85 (Q1–Q3: 51.8–68.25) during the pre-pandemic period, compared with 183.40 (Q1–Q3: 149.30–204.40) during the first peak of the pandemic (p=0.001).
Discussion: The workload levels identified in this study are consistent with those reported in similar studies. However, the specific scenario examined has scarcely been described in the existing literature.
Conclusion: The pandemic increased the nursing staff's workload threefold. A weak, direct linear correlation was identified between workload and SOFA score. The pandemic year and the presence of cardiopulmonary conditions were identified as workload predictors.
Keywords:
Nursing; COVID-19; Workload; Critical Care.
Resumen
Introducción: En los últimos años se han descrito la carga laboral de los profesionales de enfermería en unidades de cuidado intensivo. Identificar factores asociados puede contribuir a una mejor planificación del cuidado de Enfermería.
Objetivo: Determinar los predictores asociados a la carga de trabajo en enfermería de UCI en una muestra de registros tomada antes y durante el primer pico de la pandemia de COVID-19.
Materiales y Métodos: Corte transversal analítico. Se incluyeron 97 registros de pacientes de Unidades de Cuidado Intensivo. Se realizó un análisis descriptivo y multivariado, empleando una regresión lineal robusta, cuyo desenlace principal fue carga de trabajo a través del Nursing Activities Score (NAS).
Resultados: El promedio de edad fue 57,67± 17,78 y el 68,04% (n=66) eran mujeres. Se encontraron diferencias estadísticamente significativas prepandemia versus primer pico de la pandemia para variables como categoría de la enfermedad, tipo de UCI, puntaje SOFA y número de enfermeras, entre otros. (p<0,001). Se evidenció una diferencia en la mediana del puntaje del NAS 60,85(Q1:51,8- Q3:68,25) durante la pandemia versus 183,40(Q1:149,30-Q3:204,40) el primer pico, con una p=0,001.
Discusión: El nivel de carga laboral identificado en el presente estudio es equivalente a lo descrito en otros similares. Sin embargo, el escenario evaluado ha sido poco descrito en la literatura actual.
Conclusión: La pandemia triplico la cargar laboral del personal de enfermería. Se identificó una correlación lineal, directa y débil entre las cargas de trabajo y el SOFA, el año de pandemia, el tener patologías cardio-respiratorio, como factores de predicción de la carga laboral.
Palabras Clave:
Enfermería; COVID-19; Carga de Trabajo; Cuidados Críticos.
Resumo
Introdução: Nos últimos anos, tem sido descrita a carga de trabalho que os profissionais de enfermagem em unidades de terapia intensiva podem vivenciar. A identificação dos fatores associados pode contribuir para um melhor planejamento da assistência de enfermagem.
Objetivo: Determinar os preditores associados à carga de trabalho de enfermagem em UTI em uma amostra de registros obtidos antes e durante o primeiro pico da pandemia de COVID-19.
Materiais e Métodos: Estudo transversal analítico. Foram incluídos 97 registros (47 pré-pandêmicos e 50 durante o primeiro pico da pandemia) de pacientes internados em Unidades de Terapia Intensiva. Foi realizada análise descritiva e multivariada por meio de regressão linear robusta, tendo como desfecho primário a carga de trabalho mensurada pelo Nursing Activities Score (NAS).
Resultados: A média de idade foi de 57,67 ± 17,78 e 68,04% (n = 66) eram mulheres. Diferenças estatisticamente significativas foram encontradas pré-pandemia versus o primeiro pico da pandemia para variáveis como categoria da doença, tipo de UTI, SOFA e número de enfermeiros, entre outras. (p < 0,001). Uma diferença foi evidente na mediana do escore NAS 60,85 (Q1: 51,8- Q3: 68,25) durante a pandemia versus 183,40 (Q1: 149,30-Q3: 204,40) no primeiro pico, com p = 0,00.
Discussão: O nível de carga de trabalho identificado no presente estudo é equivalente ao descrito em estudos semelhantes. No entanto, o cenário avaliado tem sido pouco descrito na literatura atual.
Conclusão: A pandemia triplicou a carga de trabalho da equipe de enfermagem. Uma correlação linear fraca, direta, foi identificada entre as cargas de trabalho e o SOFA, o ano da pandemia e ter patologias cardiorrespiratórias como preditores da carga de trabalho.
Palavras-Chave:
Enfermagem; COVID-19; Carga de Trabalho; Cuidados Críticos.
Introduction
During the COVID-19 pandemic, nursing was one of the disciplines required to lead the care of patients
with COVID-19, particularly in intensive care units (ICUs)
1,2.
This care encompasses management activities (related to material, human, and financial resources),
clinical care (providing timely, comprehensive, and individualized patient care), and teaching and
research (for personnel in training and for patient and family education)
3,4.
Collectively, these activities lead to a high workload, and in recent years, even before the pandemic,
this workload has shown a consistent increasing trend
5-7.
In Colombia, it has already been demonstrated that more than half of a nursing shift may be dedicated
to a single patient, with direct care activities occupying the largest portion of that time
8.
Increased nursing workload has been described as being associated with several factors, including
hospital stays exceeding 3 days and higher Acute Physiology and Chronic Health Evaluation II
(APACHE II) scores, which classify disease severity in ICU settings. The increase has also been linked
to admissions from surgical services and diagnoses such as trauma and emergency conditions
9.
Consequently, greater patient complexity and acuity result in a higher nursing workload, which in
turn necessitates a larger number of nurses.
During the health crisis triggered by the pandemic, the number of ICU units increased while the number
of professionals remained the same, resulting in a significant impact on performance, workload, work
pressure, emotional burden, and deterioration of quality of life
10,11.
The increased nursing workload in caring for patients with COVID-19 is mainly attributable to the
specific procedures required to manage severe hypoxemia, as well as continuous monitoring and
oxygen titration for patients
12.
This panorama shows the need to understand the actual workload of ICU nursing professionals to
promote high-quality care processes under optimal working conditions for nursing staff. Accordingly,
this study aimed to identify predictors associated with ICU nursing workload using a sample of records
collected before and during the first peak of the COVID-19 pandemic.
Materials and Methods
Study Design
This was an analytical cross-sectional study.
Setting
This study was conducted in an ICU in Bucaramanga, Colombia. Pre-pandemic data were collected
between July and December 2018, and data from the first pandemic peak were collected between
February and May 2021.
Population and Sample
Non-probability sampling was employed, yielding a total of 97 patients who were assessed using
the Nursing Activities Score (NAS): 47 in the pre-pandemic period and 50 during the first peak of the
pandemic. No formal sample size calculation was performed.
Eligibility Criteria
The study included patients aged ≥18 years, selected through nonprobability sampling, who had
an ICU stay of ≥48 hours, any medical diagnosis, and a written medical order in the clinical record
to remain or continue in one of the participating ICUs (mixed, medical, surgical, or cardiovascular
units). Only patients awaiting transfer to a general ward or receiving palliative care were excluded.
The number of patients evaluated corresponded to the total monthly discharges from each unit.
Instrument and Measurements
Workload was measured using the NAS as the dependent variable. The NAS is a widely used scale for
estimating the average amount of time a professional nurse spends during a 24-hour morning shift.
It comprises seven categories subdivided into 23 activities. Each category yields a score according
to the activities included, which comprise basic activities (monitoring and control, laboratory tests,
medication, hygiene procedures, care of drains, mobilization and positioning, support and care of
relatives and patient, and administrative tasks), ventilatory support, cardiovascular support, renal
support, neurologic support, metabolic support, and specific interventions
13.
According to the authors, the NAS should be interpreted as follows
14:
- A score of 100% indicates the workload of one nurse for a 24-hour shift.
- Two patients scoring 50% each would require one full-time equivalent (FTE) nurse for the entire 24-hour shift.
- If an ICU totals 350 points in 24 hours, it requires the work of 3.5 nursing FTEs for that day.
The NAS was originally validated in 15 countries
14
and is the most widely used instrument worldwide for measuring nursing workload. It has also been
previously applied by the authors of this study in Colombia
8,9.
For this study, the NAS was recorded by a trained nurse using a paper-based form. Measurements were
performed at two time points: first in 2018 and then in 2021 during the first peak of the COVID-19
pandemic.
A specific questionnaire was used to measure the independent sociodemographic variables, including
age, sex, marital status, educational level, socioeconomic status, occupation, and social security
coverage. Additional variables of interest included the scores of the clinical predictors APACHE II and
the Sequential Organ Failure Assessment (SOFA). Variables related to the patient’s health status were
also considered, such as source of admission, diagnostic category, mortality, and length of hospital
stay. Within this set, ICU-related variables were collected, including the total number of patients, the
number of nurses per shift, the unit occupancy rate, and the ICU type.
Data Collection
Data were collected by three nurses who were duly trained by the principal investigator of the study.
At the end of each shift, they interviewed the on-duty nurse and completed the paper-based data
collection form. The authors had previously designed this form to collect sociodemographic, clinical,
predictive, ICU-related, and NAS data. Clinical information concerning the patient’s condition was
verified using the electronic medical record. The collected data were subsequently entered into a
coded Excel file, where typographical errors were checked and corrected.
Data Analysis
After data cleaning, the database was imported into STATA version 14.0 for statistical analysis. A
descriptive analysis was performed for sociodemographic, clinical, and health status variables,
stratified by data collection period (pre-pandemic vs. first pandemic peak). Continuous variables were
summarized as medians with interquartile ranges (Q1–Q3) or as means with standard deviations,
depending on the distribution of the variables, as confirmed by the Shapiro-Wilk test and skewness-
kurtosis tests (Sktest). In contrast, polytomous nominal variables were presented as absolute and
relative frequencies.
Bivariate analyses were performed by data collection period (pre-pandemic versus the first peak of
the COVID-19 pandemic). Nominal variables were compared using Pearson’s chi-square or Fisher’s
exact test. Likewise, median values were compared using the Kruskal-Wallis test or Student’s t-test
depending on the distribution of the variables.
Robust simple linear regression models were used to estimate the effect of each potential predictor on
the NAS. Additionally, robust simple linear regression models were developed for each independent
variable of interest identified from the literature and the investigators’ clinical expertise, including
age, sex, patient’s source of admission, diagnostic category, APACHE II score, ICU length of stay, and
data collection period. Spearman’s correlation coefficients were calculated for APACHE II versus SOFA
and for NAS versus APACHE II.
Finally, a robust multiple linear regression model was developed using the NAS as the outcome.
Sociodemographic variables such as gender and age, along with health status and ICU-related
factors—including patients’ source of admission, ICU length of stay, diagnostic category, APACHE II
score, data collection period, and SOFA score (both continuous and in quartiles)—were considered
as potential primary predictors. A p-value <0.05 was considered statistically significant. All statistical
tests were two-tailed. Data were analyzed using STATA 14.0 software
15.
The complete dataset is publicly available on Mendeley Data
16.
Ethical Considerations
This study complied with Resolution No. 08430 of 1993 issued by the Colombian Ministry of Health
and was classified as involving “less than minimal risk”
17.
All participants provided written informed consent. The study protocol was approved by the
institutional ethics committee (Concept No. 022-2018), Subcommittee on Bioethics, Minute No. 010,
dated May 21, 2018, and adhered to national and international regulations governing research
involving human subjects
18.
Results
The mean age of participants was 57.67 ± 17.78 years, and 68.04% (n=66) were male. Table 1 shows
statistically significant differences in nursing workload between the pre-pandemic period and the
first peak of the pandemic for the variables of education, occupation, patient’s source of admission,
discharge destination, disease category, ICU type, SOFA score, and number of nurses.
Table 1. Comparison of sociodemographic and clinical characteristics of the population before and during the first peak of the pandemic
X
Table 1. Comparison of sociodemographic and clinical characteristics of the population before and during the first peak of the pandemic
| Characteristics |
All
n = 97
% (n) |
Pre-pandemic (2018)
n = 47
% (n) |
During the first peak of the pandemic (2021)
n = 50
% (n) |
p-value |
| Age, years (mean ± SD) |
57.67 ± 17.78 |
57.40 ± 17.84 |
57.92 ± 17.9 |
0.887¥ |
| Sex |
| | |
0.388Ɨ |
| Female | 31.96 (31) | 36.17 (17) | 28.00 (14) | |
| Male | 68.04 (66) | 63.83 (30) | 72.00 (36) | |
| Marital status |
| | |
0.075Ɨ |
| Single | 34.02 (33) | 40.43 (19) | 28.00 (14) | |
| Married | 39.18 (38) | 38.3 (18) | 40.00 (20) | |
| Cohabiting | 15.46 (15) | 6.38 (3) | 24.00 (12) | |
| Divorced | 3.09 (3) | 2.13 (1) | 4.00 (2) | |
| Widow/widower | 8.25 (8) | 12.77 (6) | 4.00 (2) | |
| Socioeconomic status |
| | |
0.749Ɨ |
| Low | 27.08 (27) | 23.91 (11) | 30.00 (15) | |
| Middle | 63.54 (61) | 67.39 (32) | 60.00 (30) | |
| High | 9.38 (9) | 8.7 (4) | 10.00 (5) | |
| Educational level |
| | |
<0.001Ɨ |
| None | 3.09 (3) | 4.26 (2) | 2.00 (1) | |
| Incomplete elementary school | 12.37 (12) | 21.28 (10) | 4.00 (2) | |
| Completed elementary school | 16.49 (16) | 6.38 (3) | 26.00 (13) | |
| Incomplete secondary school | 11.34 (11) | 17.02 (8) | 6.00 (3) | |
| Completed secondary school | 24.74 (24) | 31.91 (15) | 18.00 (9) | |
| Completed technical program | 12.37 (12) | 10.64 (5) | 14.00 (7) | |
| Incomplete university education | 2.06 (2) | 4.26 (2) | 0.00 (0) | |
| Completed university education | 17.53 (17) | 4.26 (2) | 30.00 (15) | |
| Occupation |
| | |
0.005Ɨ |
| None | 32.99 (32) | 48.94 (23) | 18.00 (9) | |
| Student | 2.06 (2) | 0.00 (0) | 4.00 (2) | |
| Employee | 22.68 (22) | 17.02 (8) | 28.00 (14) | |
| Self-employed | 27.84 (27) | 21.28 (10) | 34.00 (17) | |
| Unemployed | 3.09 (3) | 6.38 (3) | 0.00 (0) | |
| Pensioner/Retired | 11.34 (11) | 6.38 (3) | 16.00 (8) | |
| Source of admission |
| | |
0.007Ɨ |
| Emergency room | 38.14 (37) | 21.28 (10) | 54.00 (27) | |
| Surgery | 3.09 (3) | 4.26 (2) | 2.00 (1) | |
| Hospitalization | 12.37 (12) | 21.28 (10) | 4.00 (2) | |
| Referral | 32.99 (32) | 38.3 (18) | 28.00 (14) | |
| Other | 13.4 (13) | 14.89 (7) | 12.00 (6) | |
| Patient discharge destination |
| | |
<0.001Ɨ |
| Morgue | 30.21 (29) | 34.78 (16) | 26.00 (13) | |
| Home | 5.21 (5) | 2.17 (1) | 8.00 (4) | |
| Hospitalization | 36.46 (35) | 56.52 (26) | 18.00 (9) | |
| General care unit | 20.83 (20) | 6.52 (3) | 34 (17) | |
| ECMO ICU | 7.29 (7) | 0.00 (0) | 14 (7) | |
| Disease category |
| | |
<0.001ƗƗ |
| Infectious | 10.31 (10) | 21.28 (10) | 0.00 (0) | |
| Metabolic | 3.09 (3) | 6.38 (3) | 0.00 (0) | |
| Central nervous system | 7.22 (7) | 14.89 (7) | 0.00 (0) | |
| Circulatory | 7.22 (7) | 14.89 (7) | 0.00 (0) | |
| Respiratory | 61.86 (60) | 21.28 (10) | 100.00 (50) | |
| Gastrointestinal | 3.09 (3) | 6.38 (3) | 0.00 (0) | |
| Connective tissue | 1.03 (1) | 2.13 (1) | 0.00 (0) | |
| Trauma | 5.15 (5) | 10.64 (5) | 0.00 (0) | |
| Intoxication | 1.03 (1) | 2.13 (1) | 0.00 (0) | |
| Type of ICU |
| | |
<0.001Ɨ |
| Intermediate | 16.67 (16) | 0 (0) | 32.00 (16) | |
| Full-care ICU | 83.33 (80) | 100 (46) | 68.00 (34) | |
| Days of ICU stay (median: Q1–Q3) |
11 [7; 16.5] |
11.5 [7; 17] |
10 [7; 15] |
0.432£ |
| Mortality (yes) |
29.90 (29) |
34.04 (16) |
26.00 (13) |
0.387Ɨ |
| APACHE II (median: Q1–Q3) |
10 [0; 18] |
--- |
10 [0; 18] |
--- |
| SOFA (mean ± SD) |
6.64 ± 4.17 |
8.13 ± 3.49 |
5.24 ± 4.29 |
0.005¥ |
| Total of patients (median: Q1–Q3) |
14 [12; 14] |
14 [13; 14] |
13 [10; 26] |
0.971£ |
| Nurses at time of assessment (median: Q1–Q3) |
4.0 [4.0; 4.0] |
4.0 [4.0; 4.0] |
4.0 [4.0; 8.0] |
<0.001£ |
| Percentage of occupancy (median: Q1–Q3) |
92.59 [76.92; 100] |
100 [85; 100] |
90.60 [74.07; 100] |
0.079£ |
| Patient/nurse ratio (median: Q1–Q3) |
3.25 [3.0; 3.5] |
3.5 [3.25; 3.5] |
3.0 [2.5; 3.25] |
<0.001£ |
SD: Standard deviation; Q: quartile; ICU: Intensive care unit; APACHE: Acute physiology and chronic health evaluation; ECMO:
Extracorporeal membrane oxygenation; ƗChi-square test for categorical variables. ƗƗFisher’s exact test. ¥Student’s t-test. £Mann–
Whitney U test.
The median NAS during the first peak of the pandemic was 183.40 (Q1: 149.30; Q3: 204.40), compared
with 60.85 (Q1: 51.80; Q3: 68.25) in the pre-pandemic period (p=0.001; Table 2).
Table 2. Comparison of the overall and activity-based NAS before and after the COVID-19 pandemic
X
Table 2. Comparison of the overall and activity-based NAS before and after the COVID-19 pandemic
| Characteristic |
All
Median (Q1–Q3) |
Pre-pandemic (2018)
Median (Q1–Q3) |
First peak of the pandemic (2021)
Median (Q1–Q3) |
p-value |
| Overall NAS |
92.75 [61.9; 184.5] |
60.85 [51.8; 68.25] |
183.40 [149.30; 204.40] |
0.001 |
| Monitoring and control |
20.35 [16.60; 36.20] |
16.60 [16.60; 20.15] |
36.20 [36.20; 36.20] |
0.001 |
| Laboratory procedures |
4.30 [4.30; 4.30] |
2.15 [2.10; 4.30] |
4.3 [4.3; 4.3] |
0.001 |
| Administrative and managerial tasks |
5.60 [5.60; 5.60] |
5.60 [5.60; 5.60] |
5.60 [5.60; 5.60] |
0.073 |
| Hygiene procedures |
12.30 [4.10; 20.60] |
4.10 [2.05; 4.10] |
20.60 [20.60; 40.60] |
0.001 |
| Care of drains |
0.0 [0.0; 1.08] |
0.0 [0.0; 0.90] |
0.0 [0.0; 1.80] |
0.021 |
| Mobilization and positioning |
17.90 [12.40; 34.90] |
12.40 [5.50; 12.40] |
34.90 [17.90; 34.90] |
0.001 |
| Support and care of relatives or patients |
4.0 [0; 4] |
0.0 [0.0; 2.0] |
4.0 [4.0; 36] |
0.001 |
| Medication administration |
4.20 [4.20; 57.40] |
4.20 [4.2; 4.20] |
57.40 [27.40; 57.40] |
0.001 |
| Ventilatory support |
5.80 [2.20; 7.60] |
2.30 [1.40; 5.40] |
7.60 [5.80; 7.60] |
0.001 |
| Cardiovascular support |
2.45 [1.20; 3.70] |
1.20 [0.6; 2.45] |
2.5 [1.2; 3.7] |
0.001 |
| Renal support |
7.0 [7.0; 7.0] |
7.0 [7.0; 7.30] |
7.0 [7.0; 7.0] |
0.017 |
| Neurologic support |
0.0 [0.0; 0.0] |
0.0 [0.0; 0.0] |
0.0 [0.0; 0.0] |
0.143 |
| Metabolic support |
1.30 [1.30; 2.60] |
1.30 [1.30; 2.80] |
1.950 [1.30; 2.60] |
0.578 |
| Specific interventions |
0.9 [0; 2.1] |
0.0 [0; 0.9] |
1.90 [0; 3.2] |
0.001 |
NAS: Nursing Activities Score; Q: quartile; ⱡKruskal–Wallis test for comparison of medians.
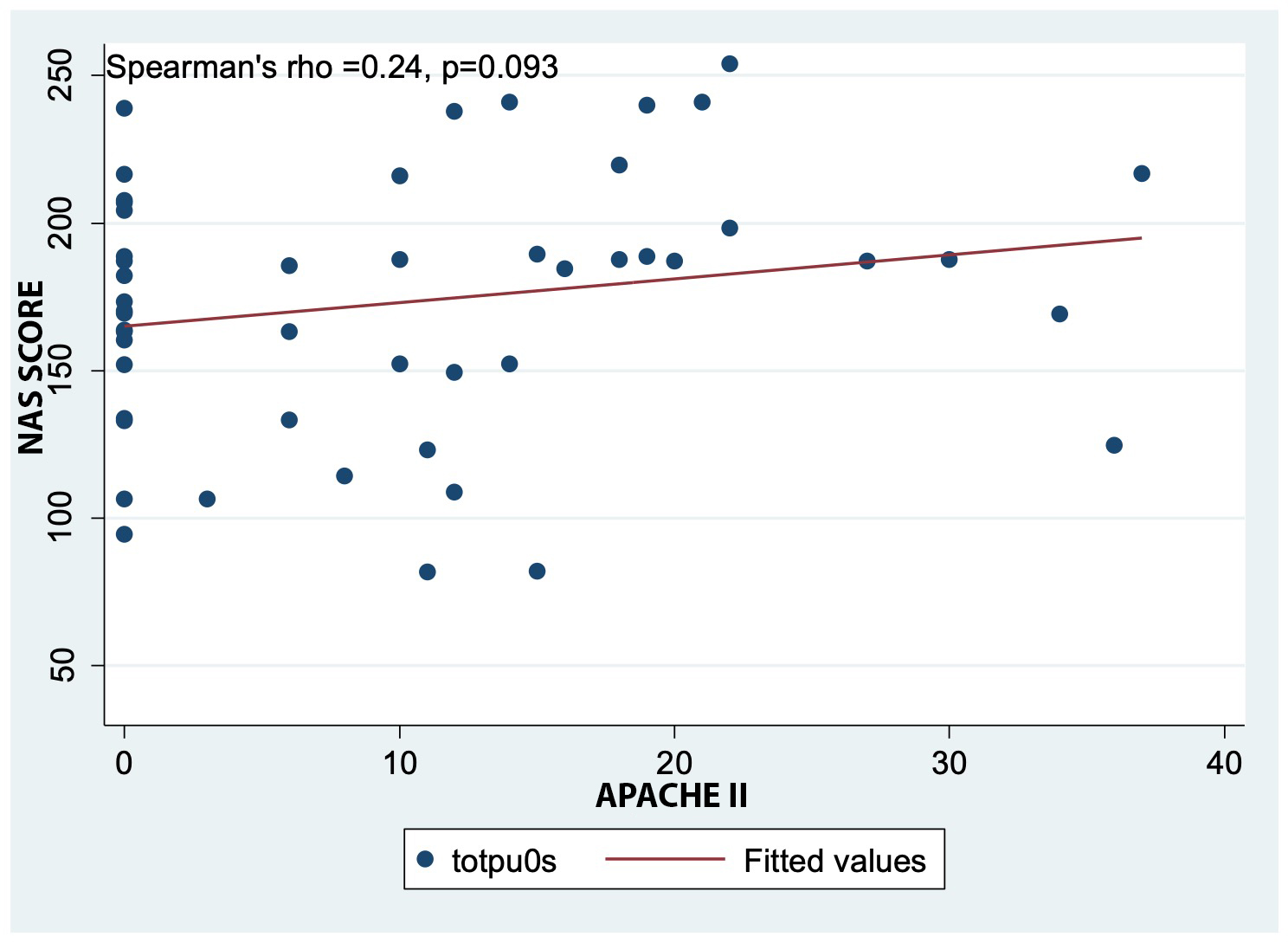
Figure 1 shows a direct but weak linear correlation between the NAS and APACHE II score. Although
this association was not statistically significant (p=0.093), it is evident that as the probability of death
increases, the nursing workload also increases.
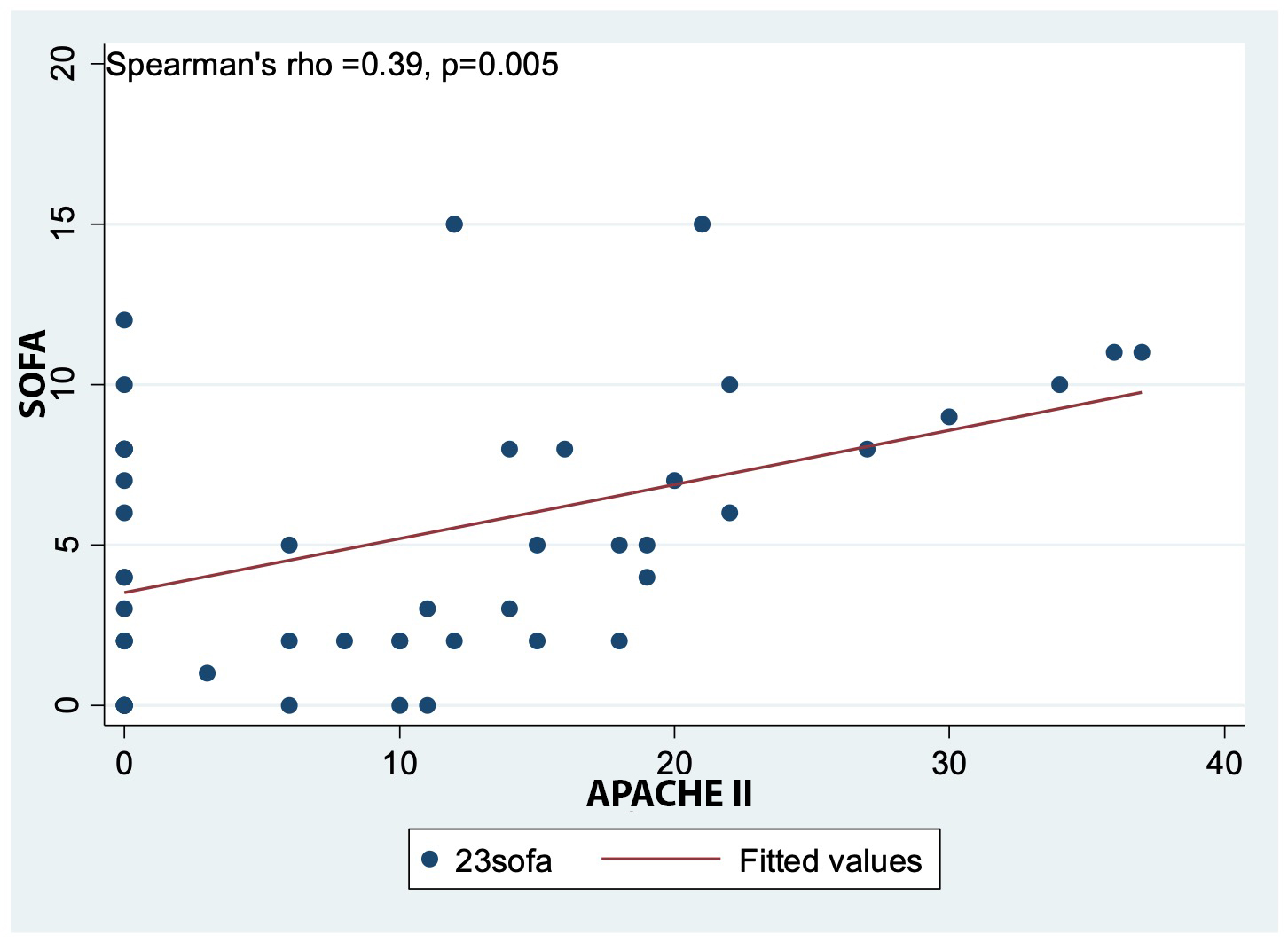
Figure 2 shows a direct but weak linear correlation between the SOFA and APACHE II scores, with
a statistically significant association (p=0.005). This indicates that as the SOFA score increases, the
APACHE II score also tends to increase.
Regarding the robust linear regression model, the main findings indicated that the SOFA score, the
pandemic year, the presence of cardiorespiratory conditions, and being a student or retired were
associated with higher NAS. In other words, these variables are predictors of nursing workload (Table 3).
Table 3. Exploratory analysis of simple and fitted predictors of workload in a robust linear regression model
X
Table 3. Exploratory analysis of simple and fitted predictors of workload in a robust linear regression model
| Nursing Activities Score (NAS) |
Simple models: Raw effects |
Final model (R2) (n=97)¥¥ |
| β |
(95% CI) |
p value¥ |
β |
(95% CI) |
p value* |
| Age (years) |
0.30 |
(-0.42 to 1.03) |
0.411 |
0.25 |
(-0.27 to 0.77) |
0.339 |
| β₀ = 101.56 |
R² = 65.06ⱡ |
(60.21 to 142.90) |
<0.001 |
|
|
|
| Sex |
|
Reference: Women |
|
|
|
|
| Sex (male) |
0.56 |
(-28.52 to 29.63) |
0.970 |
-9.77 |
(-23.24 to 3.69) |
0.153 |
| β₀ = 118.55 |
R² = 65.281 |
(93.96 to 143.14) |
<0.001 |
|
|
|
| Occupation |
|
References: None |
|
|
|
|
| Student |
81.06 |
(53.35 to 108.78) |
<0.001 |
42.81 |
(11.68 to 73.95) |
0.008 |
| Employee |
29.29 |
(-3.22 to 61.80) |
0.077 |
2.62 |
(-16.34 to 21.58) |
0.784 |
| Self-employed |
38.54 |
(6.24 to 70.84) |
0.020 |
4.09 |
(-16.49 to 24.67) |
0.693 |
| Unemployed |
-29.617 |
(-50.05 to -9.18) |
0.005 |
3.14 |
(-14.88 to 21.14) |
0.730 |
| Pensioner/Retired |
69.45 |
(21.10 to 117.81) |
0.005 |
25.09 |
(3.79 to 46.38) |
0.022 |
| β₀ = 92.93 |
R² = 61.36 |
(73.61 to 112.26) |
<0.001 |
|
|
|
| Source of admission |
|
Reference: Emergency room |
|
|
|
|
| Surgery |
-35.06 |
(-124.81 to 54.69) |
0.440 |
-10.07 |
(-28.89 to 8.76) |
0.290 |
| Hospitalization |
-58.88 |
(-91.44 to -26.32) |
0.001 |
5.60 |
(-11.32 to 22.52) |
0.512 |
| Referral |
-22.37 |
(-53.06 to 8.32) |
0.151 |
-0.36 |
(-15.05 to 14.32) |
0.961 |
| Other |
-28.02 |
(-72.84 to 16.81) |
0.218 |
-17.81 |
(-49.52 to 13.90) |
0.267 |
| β₀ = 138.44 |
R² = 63.43 |
(116.84 to 160.03) |
<0.001 |
|
|
|
| Diagnostic category |
|
Reference: Infectious-Metabolic |
|
|
|
|
| Mental sphere |
-3.14 |
(-15.65 to 9.36) |
0.619 |
-5.08 |
(-25.90 to 15.74) |
0.628 |
| Cardiovascular |
83.09 |
(66.64 to 99.54) |
<0.001 |
-14.89 |
(-31.60 to 1.819) |
0.080 |
| Gastrointestinal |
-1.92 |
(-16.67 to 12.84) |
0.797 |
-2.91 |
(-33.13 to 27.29) |
0.848 |
| Trauma and emergencies |
2.28 |
(-12.95 to 17.52) |
0.767 |
5.61 |
(-14.25 to 25.47) |
0.575 |
| β₀ = 61.67 |
R² = 53.20 |
(55.77 to 67.55) |
<0.001 |
|
|
|
| SOFA |
-2.05 |
(-5.07 to 0.98) |
0.183 |
2.48 |
(0.07 to 4.89) |
0.043 |
| β₀ = 132.52 |
R² = 64.72 |
(111.28 to 153.76) |
<0.001 |
|
|
|
| Days of stay in ICU |
-0.81 |
(-2.29 to 0.67) |
0.281 |
0.14 |
(-0.83 to 1.11) |
0.779 |
| β₀ = 129.74 |
R² = 64.93 |
(106.62 to 152.86) |
<0.001 |
|
|
|
| Type of ICU |
|
Reference: Intermediate |
|
|
|
|
| Full ICU |
-35.71 |
(-60.64 to -10.78) |
0.005 |
26.21 |
(-0.71 to 53.14) |
0.056 |
| β₀ = 149.35 |
R² = 63.89 |
(129.46 to 169.24) |
<0.001 |
|
|
|
| Health care provider location |
|
Reference: Pre-pandemic |
|
|
|
|
| Post-pandemic |
112.09 |
(99.32 to 124.86) |
<0.001 |
133 |
(115.50 to 150.50) |
<0.001 |
| β₀ = 61.156 |
R² = 32.52 |
(57.75 to 64.56) |
<0.001 |
|
|
|
CI: Confidence interval ; ¥Robust simple linear regression model; ⱡRobust simple linear regression model;¥¥Linear regression
model including age, sex, occupation, source of admission, diagnostic category, SOFA score, ICU length of stay, ICU type, and
data collection period; *p-value of the adjusted robust multiple linear regression model.
Categorization of the SOFA scale showed that as the mean point of each SOFA quartile increased,
workload measured by NAS remained approximately constant. Likewise, when comparing with the
reference quartile (first quartile) in the robust multiple regression model adjusted for other factors,
there was an average increase of 27 points in nursing workload across each subsequent SOFA quartile.
Table 4. Adjusted effect of categorized SOFA on workload as measured by NAS
X
Table 4. Adjusted effect of categorized SOFA on workload as measured by NAS
| SOFA quartile |
Average SOFA quartile score
X̄ ± SD |
Minimum of SOFA quartile |
Maximum of SOFA quartile |
NAS mean score for SOFA quartile
X̄ ± SD |
Coefficient of linear regression†
β, 95% CI |
| Quartile 1 (p25) |
1.56 ± 1.19 |
0 |
3 |
140.04 ± 50.48 |
Reference category in regression analysis |
| Quartile 2 (p50) |
5.34 ± 1.08 |
4 |
7 |
106.58 ± 65.00 |
27.06 (4.75–49.38) |
| Quartile 3 (p75) |
8.81 ± 0.92 |
8 |
10 |
117.04 ± 70.95 |
27.00 (4.77–49.24) |
| Quartile (p100) |
13.3 ± 1.95 |
11 |
17 |
111.56 ± 72.11 |
27.76 (-5.19–58.72) |
SOFA: Sequential Organ Failure Assessment Score; NAS: Nursing Activities Score; SD: Standard deviation; CI: Confidence interval;
ⱡRobust multiple linear regression adjusted for sex, age, occupation, source of admission, diagnostic category, ICU length of
stay, ICU type, and data collection period.
Discussion
This study aimed to identify predictors associated with ICU nursing workload using a sample of
records collected before and during the first peak of the COVID-19 pandemic.
During the pandemic, a considerable increase in nursing workload was observed due to the intensive
care required by patients diagnosed with COVID-19
19.
Our study analyzed clinical predictors associated with ICU nursing workload before and during the
first peak of the COVID-19 pandemic; notably, NAS tripled during this period. Furthermore, although
COVID-19 is a respiratory disease similar to many others, the nursing workload exceeded levels
observed in patients with similar diagnoses, such as pneumonia of other etiologies
20.
Among the main clinical predictors, higher APACHE II and SOFA scores were associated with higher
NAS in ICU patients in this study. However, only the SOFA score demonstrated a statistically significant
association. These findings have also been reported in ICUs from other countries. For example, the
study by Bruynel et al. in Belgium reported a significant association between increased NAS among
critically ill patients and elevated APACHE II scores (p=0.006). Other similar studies comparing NAS
with APACHE II/IV scores have also shown statistically significant relationships
20,21.
This pattern could serve as a preliminary method to identify which patients will require longer
periods of direct nursing care in units where no workload measurement tool has been established.
Similarly, in older patients, higher age correlated with higher NAS, which may be related to their
medical histories and clinical conditions, as advancing age increases the risk of complications in the
ICU
8,22.
Furthermore, we found that for every 25% increase in the SOFA score—which monitors a patient’s
condition during their ICU stay—workload increased by an average of 27 points. This finding may
guide the planning of nursing shifts and the implementation of contingency plans during periods of
maximum patient flow or peak occupancy, such as pandemics or mass influxes of critically ill patients.
Regarding disease category, few comparable studies were found. One of them, conducted in 2019,
reported a significant difference between the type of admission and the nursing workload required by
patients on the first day in the ICU (p=0.025)
23.
This finding was related to the patient acuity indicator used in that study, the Simplified Acute
Physiologic Score (SAPS), which makes it non-comparable with our study. However, both studies
indicate that there is no relationship between the patient’s source of admission and the NAS, although
our study included a larger number of admission sources.
In the robust simple linear regression model, an association between the clinical characteristics of the
patients included in the study and workload was found, particularly with cardiovascular patients and
length of stay. These findings are consistent with a Brazilian study reporting moderate correlations
between workload, length of stay, vasoactive drug use, and patient acuity
24.
Another Brazilian study involving 509 patients reported higher workloads for morning shifts, male
patients, medical treatments, and patients admitted from emergency departments or other ICUs.
Additionally, female nurses, a greater number of assigned patients, and longer ICU stays were directly
associated with higher NAS. Work in surgical and burn ICUs has been inversely correlated with NAS
25.
The number of nursing professionals was identified as a predictor associated with workload. This
finding not only indicates the need for a greater number of professionals in critical care areas but
also underscores the importance of ensuring that these professionals possess the necessary clinical
competencies to manage the care of critically ill patients effectively. In such contexts, where the
severity of the patient’s condition requires constant monitoring and rapid, accurate decision-making,
nursing competence cannot be limited to technical skills alone; it must also encompass the ability to
establish a strong and trusting therapeutic relationship with patients and their families. A relationship
grounded in effective communication and emotional support is essential for reducing patient anxiety,
enhancing care experience, and increasing adherence to treatment. Nurses who maintain consistent,
empathetic interactions with their patients can detect earlier signs of complications and changes in
their clinical condition, which is vital for timely intervention and improved clinical outcomes
26.
Measuring workloads is therefore crucial to ensure that the number of available nurses is appropriate,
enabling them to manage both the technical and emotional aspects of care properly. When nurses
are overburdened, their ability to provide comprehensive, personalized care is compromised,
directly affecting the quality of care provided. Consequently, the nurse-patient relationship becomes
weakened, vigilance decreases, and the time available to address patients’ emotional needs is
reduced. Thus, proper workload planning not only ensures that patients’ technical needs are met
but also facilitates humanized, person-centered care, resulting in improved health outcomes and
increased patient satisfaction. Ultimately, ensuring an adequate number of nurses, possessing the
necessary clinical competencies, together with appropriate workload management, are key factors
for delivering effective, safe, and empathetic critical care; these elements have a positive impact on
patient outcomes and the overall quality of healthcare services
27.
The period corresponding to the first peak of the pandemic had a clear impact on nursing workload,
as confirmed by the final linear regression model. A similar finding was reported in a study from the
Netherlands, which compared data from COVID-19 and non-COVID-19 periods and found significantly
higher NAS among patients with COVID-19 than among those with pneumonia or without COVID-19
28.
The increased workload was likely due to more intensive hygiene procedures, increased need for
mobilization and positioning, greater involvement in supporting families, and heightened respiratory
care needs.
Although not originally defined as a study objective, our findings confirmed that using workload
measurement tools, such as the NAS, helps identify needs related to ICU work dynamics and
operational functioning. In particular, NAS remains one of the most widely applied instruments for
managing nursing human resources in critical care
29.
To our knowledge, this is one of the first studies to compare nursing workload before and during the
first peak of the pandemic—a period that posed significant challenges and considerable pressure
on healthcare systems and their personnel. However, the study has limitations. The healthcare
system conditions during the two periods were markedly different, and the personnel working
in the institution may also have changed over time, potentially limiting comparability. Likewise,
the diagnostic profile differed completely between the two periods, with the pandemic period
characterized by an emergent respiratory infectious condition caused by a novel pathogen. Moreover,
the absence of a formal sample size calculation may have limited the statistical power needed to
detect certain associations that were present; therefore, a type II error cannot be ruled out. Finally, no
advanced statistical analysis, such as propensity score matching, was performed to attempt to adjust
for differences in patients’ characteristics. Future studies with larger sample sizes and conducted
across multiple centers are needed, using the types of advanced statistical techniques mentioned to
compare these historical periods.
Conclusions
The COVID-19 pandemic resulted in a threefold increase in nursing workload compared with the
pre-pandemic period. This study identified a direct but weak linear correlation between nursing
workload and the SOFA score. The pandemic year and having cardiorespiratory conditions emerged
as predictors of workload. These findings can support care management by informing decisions,
such as determining the number of nurses per patient and the level of technical support that may
be required. They also serve as an indicator of how the quality of care can be improved through
individualized approaches tailored to patients and unit characteristics.
Conflict of Interest: The authors declare no conflict of interest.
Funding: This study did not receive any specific funding.
Acknowledgments: The authors express their gratitude to the participating healthcare
institution as well as to the patients and nursing staff who generously agreed to participate in this study.
References
X
Referencias
Sriharan A, West KJ, Almost J, Hamza A. COVID-19-Related Occupational Burnout and Moral Distress among Nurses: A Rapid Scoping Review. Nurs Leadersh (Tor Ont). 2021;34(1):7-19. https://pubmed.ncbi.nlm.nih.gov/33837685/
X
Referencias
Altafin JAM, Grion CMC, Tanita MT, Festti J, Cardoso LTQ, Veiga CFF, et al. Nursing Activities Score e carga de trabalho em unidade de terapia intensiva de hospital universitário. Rev bras ter intensiva. 2014;26(3):292–8. https://doi.org/10.5935/0103-507X.20140041
X
Referencias
Cáceres Rivera DI, Torres CC, Cristancho Zambrano LY, López Romero LA. Carga laboral de los profesionales de enfermería en unidad de cuidados intensivos. Estudio descriptivo: «CARETIME». Acta Colomb Cuid Intensivo. 2020;20(2):92-7. https://doi.org/10.1016/j.acci.2019.12.002
X
Referencias
Bruyneel A, Gallani MC, Tack J, d’Hondt A, Canipel S, Franck S, et al. Impact of COVID-19 on nursing time in intensive care units in Belgium. Intensive Crit Care Nurs. 2021;62:102967. https://doi.org/10.1016/j.iccn.2020.102967
X
Referencias
Phua J, Weng L, Ling L, Egi M, Lim CM, Divatia JV, et al. Intensive care management of coronavirus disease 2019 (COVID-19): challenges and recommendations. Lancet Respir Med. 2020;8(5):506-517. https://pubmed.ncbi.nlm.nih.gov/32272080/
X
Referencias
Lucchini A, Villa M, Del Sorbo A, Pigato I, D'Andrea L, Greco M, et al. Determinants of increased nursing workload in the COVID-era: A retrospective analysis of prospectively collected data. Nurs Crit Care. 2024;29(1):196-207. https://pubmed.ncbi.nlm.nih.gov/36717119/
X
Referencias
Padilha KG, Stafseth S, Solms D, Hoogendoom M, Monge FJC, Gomaa OH, et al. Nursing Activities Score: an updated guideline for its application in the Intensive Care Unit. Rev esc enferm USP. 2015;49(spe):131–7. https://doi.org/10.1590/S0080-623420150000700019
X
Referencias
StataCorp. Stata statistical software for data science. College Station, Texas; [Internet] 2003. [Cited 2020 March 25]. Available from: https://www.stata.com
X
Referencias
Hoogendoorn ME, Brinkman S, Bosman RJ, Haringman J, de Keizer NF, Spijkstra JJ. The impact of COVID-19 on nursing workload and planning of nursing staff on the Intensive Care: A prospective descriptive multicenter study. Int J Nurs Stud. 2021;121:104005. https://pubmed.ncbi.nlm.nih.gov/34273806/
X
Referencias
Silveira AT, Hohenreuther R, Schmidt NP, Silveira TT, Henz AC, Filho EMR, et al. Nursing team workload and the Apache Index of Gravity of patients post liver transplantation: A cohort study. Transplant Proc. 2022;54(8):2295-2300. https://pubmed.ncbi.nlm.nih.gov/36229278/
X
Referencias
Romano JL, Garcia PC, Silva DV, Moura BRS, de Souza Nogueira L. Type of admission and nursing workload of critical patients: a cross-sectional study. Nurs Crit Care. 2019;24(6):387-91. https://pubmed.ncbi.nlm.nih.gov/31294518/
X
Referencias
Amadeu LM, Dell’Acqua MCQ, Castro MCN, Palhares V de C, Serafim CTR, Trettene A dos S. Nursing workload in burn intensive care unit. Rev Bras Enferm. 2020;73:e20190446. https://doi.org/10.1590/0034-7167-2019-0446
X
Referencias
Moghadam KN, Chehrzad MM, Masouleh SR, Mardani A, Maleki M, Akhlaghi E, et al. Nursing workload in intensive care units and the influence of patient and nurse characteristics. Nurs Crit Care. 2021;26(6):425-31. https://doi.org/10.1111/nicc.12548
X
Referencias
Acosta-Romo MF, Maya-Pantoja GJ. Competencias clínicas y carga laboral de Enfermería en Unidades de Cuidado Intensivo Adultos. Rev Cienc Cuid. 2020;17(2):22-32. https://doi.org/10.22463/17949831.1698
X
Referencias
Hoogendoorn ME, Brinkman S, Bosman RJ, Haringman J, de Keizer NF, Spijkstra JJ. The impact of COVID-19 on nursing workload and planning of nursing staff on the Intensive Care: A prospective descriptive multicenter study. Int J Nurs Stud. 2021;121:104005. https://doi.org/10.1016/j.ijnurstu.2021.104005
X
Referencias
Cáceres Rivera DI, Ruiz Sandoval JP, Cristancho Zambrano LY, Pulido Montes MA, López Romero LA. Métodos empleados para cuantificar la carga de trabajo en Enfermería en las unidades de cuidados intensivos: una revisión de la literatura. Revista Cuidarte. 2022;13(3). https://revistas.udes.edu.co/cuidarte/article/view/2301
Sriharan A, West KJ, Almost J, Hamza A. COVID-19-Related Occupational Burnout and Moral Distress among Nurses: A Rapid Scoping Review. Nurs Leadersh (Tor Ont). 2021;34(1):7-19. https://pubmed.ncbi.nlm.nih.gov/33837685/
Fuentes GP. Enfermería y COVID-19: reconocimiento de la profesión en tiempos de adversidad. Revista Colombiana de Enfermería. 2020;19(1):e017. https://doi.org/10.18270/rce.v19i1.2970
Scholtz S, Nel EW, Poggenpoel M, Myburgh CPH. The Culture of Nurses in a Critical Care Unit. Global Qualitative Nursing Research. 2016;3. https://doi.org/10.1177/2333393615625996
Navarro-Arnedo JM, Orgiler-Uranga PE, Marín S de H. Guía práctica de enfermería en el paciente crítico. Enferm Intensiva. 2005;16(1):15-22. https://doi.org/10.1016/S1130-2399(05)73381-2
Altafin JAM, Grion CMC, Tanita MT, Festti J, Cardoso LTQ, Veiga CFF, et al. Nursing Activities Score e carga de trabalho em unidade de terapia intensiva de hospital universitário. Rev bras ter intensiva. 2014;26(3):292–8. https://doi.org/10.5935/0103-507X.20140041
Almenyan AA, Albuduh A, Al-Abbas F. Effect of nursing workload in intensive care units. Cureus. 2021;13(1):e12674. https://www.cureus.com/articles/49702-effect-of-nursing-workload-in-intensive-care-units
Ravanbakhsh E, Mahmood M, Mehrdad A, Mahdi A. A systematic review of the workload of nurses in intensive care units using NAS. Acta Med Mediterr. 2015;31(7):1455-60. https://www.researchgate.net/publication/291834877_A_systematic_review_of_the_workload_of_nurses_in_intensive_care_units_using_nas
Cáceres Rivera DI, Torres CC, Cristancho Zambrano LY, López Romero LA. Carga laboral de los profesionales de enfermería en unidad de cuidados intensivos. Estudio descriptivo: «CARETIME». Acta Colomb Cuid Intensivo. 2020;20(2):92-7. https://doi.org/10.1016/j.acci.2019.12.002
Rivera DIC, Torres CC, Romero LAL. Factors associated with nursing workload in three intensive care units. Rev esc enferm USP. 2021;55:e20200272. https://doi.org/10.1590/1980-220X-REEUSP-2020-0272
Bruyneel A, Gallani MC, Tack J, d’Hondt A, Canipel S, Franck S, et al. Impact of COVID-19 on nursing time in intensive care units in Belgium. Intensive Crit Care Nurs. 2021;62:102967. https://doi.org/10.1016/j.iccn.2020.102967
Phua J, Weng L, Ling L, Egi M, Lim CM, Divatia JV, et al. Intensive care management of coronavirus disease 2019 (COVID-19): challenges and recommendations. Lancet Respir Med. 2020;8(5):506-517. https://pubmed.ncbi.nlm.nih.gov/32272080/
Lucchini A, Villa M, Del Sorbo A, Pigato I, D'Andrea L, Greco M, et al. Determinants of increased nursing workload in the COVID-era: A retrospective analysis of prospectively collected data. Nurs Crit Care. 2024;29(1):196-207. https://pubmed.ncbi.nlm.nih.gov/36717119/
Padilha KG, Stafseth S, Solms D, Hoogendoom M, Monge FJC, Gomaa OH, et al. Nursing Activities Score: an updated guideline for its application in the Intensive Care Unit. Rev esc enferm USP. 2015;49(spe):131–7. https://doi.org/10.1590/S0080-623420150000700019
Miranda DR, Nap R, de Rijk A, Schaufeli W, Iapichino G; TISS Working Group. Nursing activities score. Crit Care Med. 2003;31(2):374-82. https://doi.org/10.1097/01.CCM.0000045567.78801.CC
StataCorp. Stata statistical software for data science. College Station, Texas; [Internet] 2003. [Cited 2020 March 25]. Available from: https://www.stata.com
Torres CC, Cáceres D, Alberto L. Base de datos. CARETIME análisis longitudinal antes y después de pandemia COVID-19. Mendeley Data V1. 2024. https://data.mendeley.com/datasets/hktp4p86c6/1
Ministerio de Salud. Resolución 8430 de 1993 Por la cual se establecen las normas científicas, técnicas y administrativas para la investigación en salud. Colombia; 1993. Disponible en: https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/DE/DIJ/RESOLUCION-8430-DE-1993.P
Asociación Médica Mundial. Declaración de Helsinki de la AMM: principios éticos para las investigaciones médicas en seres humanos. Córdoba; 2008. Disponible en: http://www.wma.net/es/30publications/10policies/b3/17c_es.pdf
Lucchini A, Giani M, Elli S, Villa S, Rona R, Foti G. Nursing Activities Score is increased in COVID-19 patients. Intensive Crit Care Nurs. 2020;59:102876. https://doi.org/10.1016/j.iccn.2020.102876
Hoogendoorn ME, Brinkman S, Bosman RJ, Haringman J, de Keizer NF, Spijkstra JJ. The impact of COVID-19 on nursing workload and planning of nursing staff on the Intensive Care: A prospective descriptive multicenter study. Int J Nurs Stud. 2021;121:104005. https://pubmed.ncbi.nlm.nih.gov/34273806/
Silveira AT, Hohenreuther R, Schmidt NP, Silveira TT, Henz AC, Filho EMR, et al. Nursing team workload and the Apache Index of Gravity of patients post liver transplantation: A cohort study. Transplant Proc. 2022;54(8):2295-2300. https://pubmed.ncbi.nlm.nih.gov/36229278/
Lozano Y, Palacios EV. Factores asociados a la hospitalización de pacientes con COVID-19 en la Unidad de Cuidados Intensivos de una clínica en 2020. Horizonte Médico (Lima). 2021;21(1). http://dx.doi.org/10.24265/horizmed.2021.v21n1.09
Romano JL, Garcia PC, Silva DV, Moura BRS, de Souza Nogueira L. Type of admission and nursing workload of critical patients: a cross-sectional study. Nurs Crit Care. 2019;24(6):387-91. https://pubmed.ncbi.nlm.nih.gov/31294518/
Amadeu LM, Dell’Acqua MCQ, Castro MCN, Palhares V de C, Serafim CTR, Trettene A dos S. Nursing workload in burn intensive care unit. Rev Bras Enferm. 2020;73:e20190446. https://doi.org/10.1590/0034-7167-2019-0446
Moghadam KN, Chehrzad MM, Masouleh SR, Mardani A, Maleki M, Akhlaghi E, et al. Nursing workload in intensive care units and the influence of patient and nurse characteristics. Nurs Crit Care. 2021;26(6):425-31. https://doi.org/10.1111/nicc.12548
Vargas-Escobar LM, Aya Roa KJ, Ortiz Mayorga JL, Quiñonez Mora MA, Hernández Bohórquez LM, Fuentes Bermúdez GP, et al. Carga del cuidado de enfermería: un análisis de concepto. Revista Cuidarte. 2024;15(3). https://revistas.udes.edu.co/cuidarte/article/view/3848
Acosta-Romo MF, Maya-Pantoja GJ. Competencias clínicas y carga laboral de Enfermería en Unidades de Cuidado Intensivo Adultos. Rev Cienc Cuid. 2020;17(2):22-32. https://doi.org/10.22463/17949831.1698
Hoogendoorn ME, Brinkman S, Bosman RJ, Haringman J, de Keizer NF, Spijkstra JJ. The impact of COVID-19 on nursing workload and planning of nursing staff on the Intensive Care: A prospective descriptive multicenter study. Int J Nurs Stud. 2021;121:104005. https://doi.org/10.1016/j.ijnurstu.2021.104005
Cáceres Rivera DI, Ruiz Sandoval JP, Cristancho Zambrano LY, Pulido Montes MA, López Romero LA. Métodos empleados para cuantificar la carga de trabajo en Enfermería en las unidades de cuidados intensivos: una revisión de la literatura. Revista Cuidarte. 2022;13(3). https://revistas.udes.edu.co/cuidarte/article/view/2301