Rev Cuid. 2026; 17(1): 5160
Abstract
Introduction: Medication administration in intensive care units is one of the main care activities of nursing professionals. The integration of scientific knowledge, together with the use of technologies such as infusion pumps, enables the reduction of errors and improves the quality of care. Objective: To describe the use of an infusion pump monitoring platform for medication administration in adult intensive care units at a university hospital in Bogotá, Colombia. Materials and Methods: This was an observational, retrospective study that collected 35,738 medication administration records from five intensive care units using a monitoring platform during 2023. A descriptive analysis was performed using frequencies and proportions, along with simple associations assessing compliance between medications and doses. Results: Compliance with the drug library during the first year of the platform was 66%. The platform reported 5,589 hard-limit blocks involving high-alert medications, of which 76% were related to the administration of noradrenaline, midazolam, and fentanyl. Discussion: The results were consistent with other studies, demonstrating drug library compliance ranging from 65% to 80% during the first year of implementation. Conclusion: The implementation of institutional medication administration monitoring programs, using technologies integrated into infusion pumps, positively impacts patient safety, reduces costs associated with care, and continuous improvement within institutions.
Keywords: Medication Therapy Management; Infusión Pumps; Patient Safety; Health Information Interoperability; Critical Care Nursing.
Resumen
Introducción: La administración de medicamentos en unidades de cuidado intensivo constituye una de las principales actividades del cuidado en los profesionales de enfermería. La integración de conocimientos científicos, sumado al uso de tecnologías como bombas de infusión, permiten reducir errores y mejorar la calidad de la atención. Objetivo: Describir el uso de una plataforma de seguimiento de bombas de infusión en la administración de medicamentos en unidades de cuidado intensivo adulto de un Hospital Universitario de Bogotá, Colombia. Materiales y Métodos: Estudio observacional, retrospectivo, el cual recolectó 35.738 registros de administración de medicamentos en cinco unidades de cuidado intensivo a través del uso de una plataforma de seguimiento durante el año 2023. Se realizó un análisis descriptivo utilizando frecuencias y proporciones, además de asociaciones simples de cumplimiento entre medicamentos versus dosis. Resultados: El cumplimiento a la biblioteca de medicamentos durante el primer año de la plataforma fue del 66%. La plataforma informó de 5.589 retrocesos en medicamentos de alto riesgo, de los cuales el 76% se relacionó con la administración de noradrenalina, midazolam y fentanilo. Discusión: Los resultados fueron consistentes con otros estudios, demostrando un cumplimiento a la biblioteca de medicamentos entre el 65% y 80% en su primer año de implementación. Conclusión: La implementación de programas institucionales de seguimiento a la administración de medicamentos, mediante el uso de tecnologías integradas a las bombas de infusión, permiten impactar positivamente la seguridad del paciente, reducir costos asociados a la atención y fortalecer la mejora continua de las instituciones.
Palabras Clave: Administración del Tratamiento Farmacológico; Bombas de Infusión; Seguridad del Paciente; Interoperabilidad de la Información en Salud; Enfermería de Cuidados Críticos.
Resumo
Introdução: A administração de medicamentos em unidades de terapia intensiva é uma das principais atividades assistenciais dos profissionais de enfermagem. A integração do conhecimento científico, aliada ao uso de tecnologias como bombas de infusão, permite reduzir erros e melhorar a qualidade do cuidado. Objetivo: Descrever o uso de uma plataforma de monitoramento de bombas de infusão na administração de medicamentos em unidades de terapia intensiva para adultos de um Hospital Universitário em Bogotá, Colômbia. Materiais e Métodos: Este foi um estudo retrospectivo e observacional que coletou 35.738 registros de administração de medicamentos em cinco unidades de terapia intensiva por meio do uso de uma plataforma de monitoramento durante o ano de 2023. Foi realizada uma análise descritiva utilizando frequências e proporções, bem como associações simples de adesão entre medicamentos e doses. Resultados: A adesão à biblioteca de medicamentos durante o primeiro ano de uso da plataforma foi de 66%. A plataforma relatou 5.589 recalls de medicamentos de alto risco, 76% dos quais relacionados à administração de norepinefrina, midazolam e fentanil. Discussão: Os resultados foram consistentes com outros estudos, demonstrando adesão da biblioteca de medicamentos entre 65% e 80% no primeiro ano de implementação. Conclusão: A implementação de programas institucionais de monitoramento da administração de medicamentos, utilizando tecnologias integradas a bombas de infusão, pode impactar positivamente a segurança do paciente, reduzir os custos associados ao cuidado e fortalecer a melhoria contínua nas instituições.
Palavras-Chave: Administração de Tratamento Farmacológico; Bombas de Infusão; Segurança do Paciente; Interoperabilidade da Informação em Saúde; Enfermagem de Cuidados Críticos.
Introduction
Before the 1970s, medications were administered via gravity infusion, a method in which the drip rate depended on gravitational force and was manually regulated1. Subsequently, conventional infusion pumps were developed that allowed infusion rates to be programmed only in ml/h and were intended for use in the administration of parenteral nutrition and cardiovascular medications1,2.
At the end of the 20th century, the Dose Error Reduction System (DERS) was integrated into infusion pumps. This integration was considered by the Emergency Care Research Institute (ECRI) in 2002 a requirement for the acceptance and recommendation of smart infusion pumps in intravenous medication administration therapy3. With this technological advance, infusion pumps could now support end users during medication infusion programming through the customization of drug libraries2. The advantages of this integrated software, within the framework of the National Patient Safety Goals proposed by the Joint Commission, include enabling the standardization of parameters related to concentration, safe dosing ranges, doses per unit of time, and duration for continuous and intermittent infusions of medications strategically prioritized by the medical center, as well as incorporating an alert system that notifies end users when programming falls outside the established limits2,4-6.
Smart infusion pumps are considered biomedical devices that integrate embedded software capable of hosting drug libraries, providing dose calculation support, and generating alerts for incorrect prescriptions, calculation errors, and programming errors1. These pumps enable systematic and objective data capture, thereby supporting the safe administration of medications. However, implementing smart pumps has been considered an arduous and complex process2,4.
Smart pump technology benefits patient safety and the healthcare professionals involved6. These advanced infusion devices create a controlled environment for the safe administration of medications through the appropriate use of drug libraries and the standardization of concentrations. By establishing precise programming of infusion rate and dose within safe limits, the risk of calculation errors made by staff and the incidence of adverse events among patients in clinical care settings, such as intensive care units, surgical services, and pediatrics, are minimized2,5,7. Among other safety-related benefits, smart infusion pumps allow the integration of multiple interoperable technological systems, which in turn enable data analysis aimed at identifying areas for improvement, accurate recording of medication infusion data in the medical record, automatic programming of infusions from the electronic health record, and coordination of infusion therapy through the use of barcodes5,8.
Adopting interoperable smart infusion pumps with monitoring software encounters technical and organizational barriers, such as outdated drug libraries due to delayed updates, ineffective alerts, usability issues, alarm fatigue, insufficient training, and a lack of clear processes for drug library management. These limitations, described across different hospital settings, are associated with low DERS compliance, equipment variability, and preventable safety risks. In contrast, interoperability and data analysis have been shown to reduce errors and improve efficiency, although they require context-specific implementation strategies. The absence or incomplete implementation of these technologies perpetuates medication errors, limits the prevention of adverse events, reduces efficiency, and increases healthcare costs3,9-11.
A limiting factor in the implementation of smart infusion pumps has been low drug library compliance. In addition, a recurring pattern of alert overrides has been observed, reflecting low user acceptance of these devices and highlighting the imperative need to integrate smart pumps with other technological systems10,11. This integration or interoperability between technological systems and infusion pumps is known as a “closed loop” medication management system and has been considered the latest innovation in safe medication administration. It ensures the interception of errors not only during programming, but also throughout medication administration, prescription, and transcription2,5,10,12,13.
Smart infusion pumps configured independently, despite incorporating DERS, may be affected by errors related to incorrect programming (based on preset dosing ranges), incorrect doses (that do not match the prescription order), incorrect medications, wrong patient selection, or incorrect administration instructions. In addition, smart pumps cannot detect changes in the patient's clinical condition, anticipated transfer orders, or unintentional changes in the concentration of a medication solution8,14,15.
Considering the above, it is evident that the implementation of smart infusion pumps involves adapting hospital infrastructure, supervising their use, ensuring adequate time availability, securing the engagement of multidisciplinary staff responsible for drug library standardization, and promoting effective communication between teams, in addition to ongoing operational and labor costs, which together may limit their benefits across different clinical units3,9.
The objective of this study was to describe the use of an infusion pump monitoring platform for medication administration in adult intensive care units (ICUs) at a university hospital in Bogotá, Colombia
Materials and Methods
This was an observational, retrospective study with an analytical approach. The study population consisted of medication administration records collected through a smart infusion pump monitoring platform (IQ Enterprise®, BAXTER Laboratories), which enables the systematic interoperability of drug library data for patients treated at a tertiary University Hospital.
IQ Enterprise® is an essential tool for monitoring and continuously improving quality-of-care standards related to safe medication administration and has been available at the university hospital since late 2022. The sample was identified using this specialized software through non-probability convenience sampling, which included all infusion data administered via smart pumps for which information was available in the IQ Enterprise® across five adult ICUs: Medical ICU, Transplant ICU, Surgical ICU (Qx), Cardiovascular ICU (CV), and Coronary ICU (CC). A record of 35,738 medication infusions administered during the 12 months of 2023 was obtained, excluding other clinical care services. The sample was categorized into two main groups according to the drug library configured in the smart infusion pumps: the Medical/Transplant ICU group with 19,529 infusions and the Qx/CV/CC ICU group with 16,209 infusions.
For data analysis, a descriptive analysis was conducted using data extracted and exported from the IQ Enterprise® software, considering the number and type of infusions administered, and the percentages of compliance with drug libraries. Data were presented in tables using descriptive measures such as frequencies and proportions. Bar charts and scatter plots were used, depending on the data distribution, to display simple associations between key variables, such as medication type and compliance with dosing limits. Data were organized and analyzed using Microsoft Excel© and SPSS Statistics (Version 25). All collected data are freely available for access in Mendeley Data16.
Ethical considerations: This study was approved by the Research and Ethics Committee of the Fundación Cardioinfantil – LaCardio (Minutes No. 037, October 16, 2024).
Results
The university hospital, Fundación Cardioinfantil–LaCardio, has five high-complexity adult ICUs and 67 beds available for the care of critically ill patients. Through the implementation and monitoring of the IQ Enterprise® software, data were exported that enabled the classification of the number of infusions administered across different adult ICUs, as well as the categorization of high-alert medications and antibiotics Table 1.
Table 1. Number of infusions per medication group
X
Table 1. Number of infusions per medication group
| Medication groups |
Intensive Care Units |
Medications |
Number of infusions |
| Vasoactive agents |
Medical/Transplant ICU |
Noradrenaline: 852 Vasopressin: 260 Adrenaline: 75 |
1,187 |
| Qx/CV/CC ICU |
Noradrenaline: 1068 Vasopressin: 488 Adrenaline: 33 |
1,589 |
| Inotropic agents |
Medical/Transplant ICU |
Dopamine: 7 Dobutamine: 66 Milrinone: 13 Levosimendan: 30 |
116 |
| Qx/CV/CC ICU |
Dopamine: 1 Dobutamine: 343 Milrinone: 166 Levosimendan: 139 |
649 |
| Sedatives and analgesics |
Medical/Transplant ICU |
Midazolam: 331 Propofol: 181 Dexmedetomidine: 389 Fentanyl: 438 Remifentanil: 100 |
1,439 |
| Qx/CV/CC ICU |
Midazolam: 260 Propofol: 105 Dexmedetomidine: 436 Fentanyl: 442 Remifentanil: 5 |
1,248 |
| Neuromuscular relaxants |
Medical/Transplant ICU |
Cisatracurium: 119 |
119 |
| Qx/CV/CC ICU |
Cisatracurium: 37 |
37 |
| Antibiotics |
Medical/Transplant ICU |
3,591 infusions |
4,580 |
| Qx/CV/CC ICU |
989 infusions |
Source: © 2024 Baxter. All rights reserved. Baxter and IQ Enterprise Connectivity Suite are registered trademarks of Baxter International Inc. Data exported by: [USER] on November 15, 2024, at 11:42:19 a.m. ICU: Intensive Care Unit, Qx/CV/CC ICU: Surgical, Cardiovascular, and Coronary Intensive Care Units.
DERS compliance, referring to the drug library configured in the smart infusion pumps, was determined, as opposed to the basic mode, which consists of standard programming that does not allow identification of the medication being administered. During the first year of implementation and use of data interoperability, an overall compliance rate of 66% was observed across the institution's adult ICUs. The platform enabled visualization of overrides and hard-limit blocks, which refer to the number of times an operator performed or attempted to perform modifications to previously established parameters for different medications (soft and hard limits), with a total of 15,584 events identified. Overrides correspond to actions to modify medication doses outside standardized limits and do not affect the patient's health (soft limits), whereas hard-limit blocks are system-configured blocking actions (hard limits) that restrict dose adjustments for high-alert medications, thereby preventing patient harm Table 2.
Table 2. Drug library compliance
X
Table 2. Drug library compliance
| Service area |
Number of infusions (n=35,738) |
DERS % 66.06 (n=23,609) |
Basic mode % 33.94 (n=12,129) |
Overrides % 27.96 (n=9,995) |
Hard-limit blocks % 15.63 (n=5,589) |
| Medical/Transplant ICU |
19,529 |
67.21 (13,125) |
32.79 (6,404) |
61.14 (6,110) |
44.93 (2,511) |
| Qx/CV/CC ICU |
16,209 |
64.68 (10,484) |
35.32 (5,725) |
38.86 (3,885) |
55.07 (3,078) |
Source: © 2024 Baxter. All rights reserved. Baxter and IQ Enterprise Connectivity Suite are registered trademarks of Baxter International Inc. Data exported by: [USER] on November 15, 2024, at 11:42:19 a.m. DERS: Dose error-reduction system, ICU: Intensive Care Unit, Qx/CV/CC ICU: Surgical, Cardiovascular, and Coronary Intensive Care Units.
High-alert medications were classified as vasoactive agents, inotropic agents, sedatives and analgesics, and neuromuscular relaxants Table 3. Among these, a notable percentage of hard-limit blocks was observed by midazolam (40.52%), fentanyl (20.73%), and noradrenaline (14.88%).
Table 3. Overrides and hard-limit blocks by medication (n=4,905)
X
Table 3. Overrides and hard-limit blocks by medication (n=4,905)
| Medication groups |
Medications |
Overrides % 63.02 (n=3,091) |
Hard-limit blocks % 36.98 (n=1,814) |
| Vasoactive agents |
Noradrenaline Vasopressin Adrenaline |
20.96 (648) 11.91 (368) 1.49 (46) |
14.88 (270) 3.91 (71) 1.21 (22) |
| Inotropic agents |
Dopamine Dobutamine Milrinone Levosimendan |
0.91 (28) 17.99 (556) 2.33 (72) 0.03 (1) |
0.44 (8) 2.04 (37) 1.38 (25) 0.61 (11) |
| Sedatives and analgesics |
Midazolam Propofol Dexmedetomidine Fentanyl Remifentanil |
0.55 (17) 11.74 (363) 9.64 (298) 19.86 (614) 1.33 (41) |
40.52 (735) 4.69 (85) 8.16 (148) 20.73 (376) 0.77 (14) |
| Neuromuscular relaxants |
Cisatracurium |
1.26 (39) |
0.66 (12) |
Source: © 2024 Baxter. All rights reserved. Baxter and IQ Enterprise Connectivity Suite are registered trademarks of Baxter International Inc. Data exported by: [USER] on November 15, 2024, at 11:42:19 a.m.
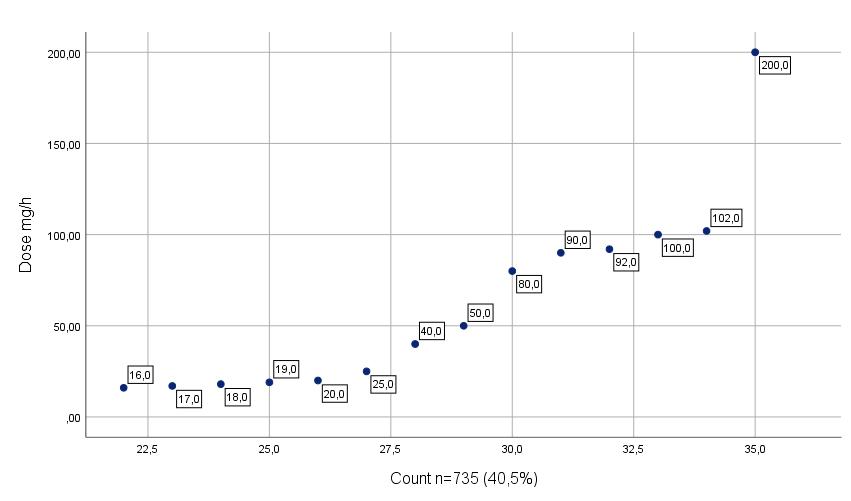
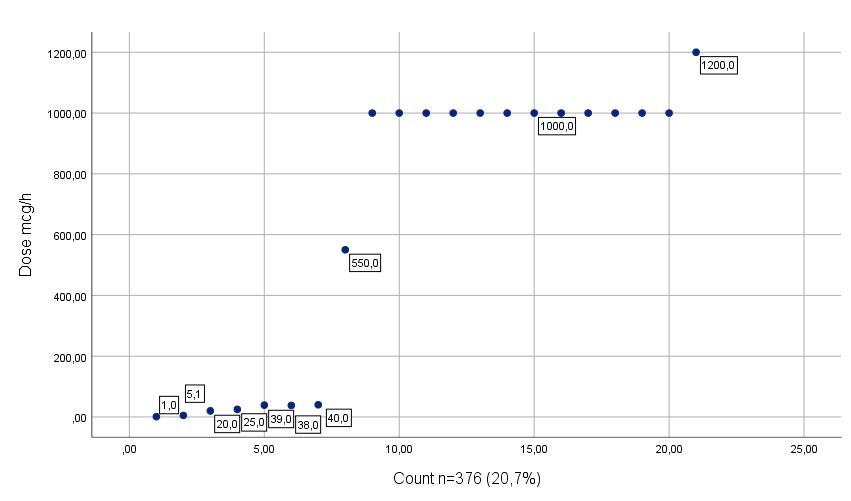
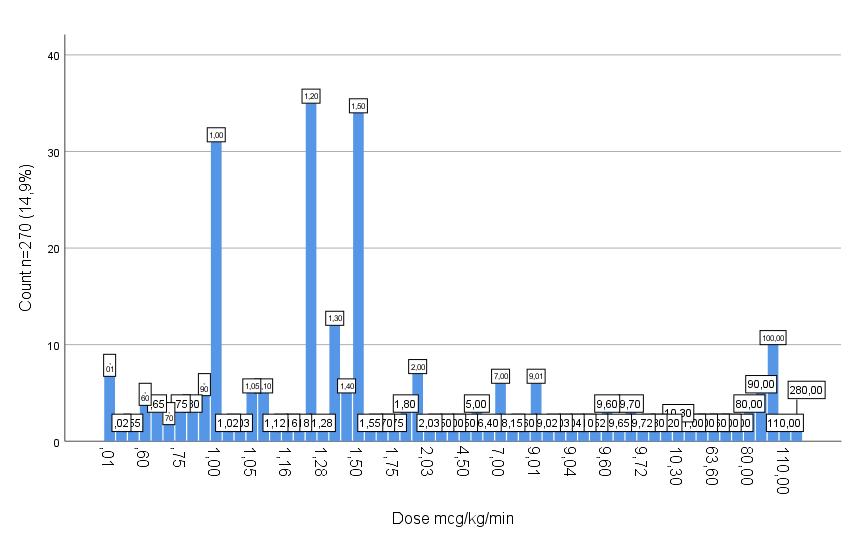
With regard to hard-limit blocks, the configuration of smart infusion pumps enabled the prevention of dosing errors involving high-alert medications, including those under special control. Considering attempts to exceed upper hard limits, it was identified that, for midazolam, the maximum configured dose was 15 mg/h, while the highest attempted dose resulting in a hard-limit block was 200 mg/h. For fentanyl, the established threshold was set at up to 500 mcg/h, with programming attempts ranging from 550 to 1200 mcg/h. For vasopressors, such as noradrenaline, the maximum permitted dose was 0.8 mcg/kg/min, with programming attempts ranging from 0.9 to 280 mcg/kg/min observed in the programming records.
Finally, Figures 1, 2, and 3 show the most relevant hard-limit blocks in high-alert medications identified through the monitoring platform.
Discussion
This study has demonstrated that the use of smart infusion pumps integrated with interoperable data-monitoring and analysis systems positively impacts patient safety. The results were consistent with existing literature at global and national levels, demonstrating drug library compliance ranging from approximately 65% to 80% during the first year of implementation; however, compliance may vary15,17.
The safe administration of medications in highly complex settings such as ICUs poses a challenge for professional nursing practice. For this reason, the implementation and adoption of technological tools that help minimize errors play a relevant role in clinical care. Previous studies have shown that ICUs are settings characterized by specialized care for complex patients, thereby generating significant demand for care, particularly the administration of multiple intravenous medications, including high-alert medications such as vasopressors, inotropic agents, sedatives, among other agents15,18.
Similar studies conducted in ICUs have reported the most relevant alerts, with vasoactive and sedative medications being of greatest concern. The findings confirm that high-alert medications such as noradrenaline, as well as certain specially controlled medications, such as midazolam and fentanyl, warrant particular attention, especially during dose titration. Through the integration of smart infusion pumps into a Dose Error Reduction System using the IQ Enterprise® software, a 76% prevention in potential adverse events related to doses exceeding those reported in the literature and in institutional protocols was demonstrated19.
Globally, numerous studies have linked technology to the prevention of medication administration errors; however, in Colombia, few studies have focused on analyzing this phenomenon13. Despite consistent in terms of compliance and potential errors prevented through technology, the results of this study raise concerns regarding a fundamental competency of nursing professionals, namely the safe administration of medications. Previous data suggest an incidence of errors in intravenous medication administration ranging from 49% to 81%, with ICUs representing one of the areas with the greatest contribution due to the high number of infusions administered, as well as the relationship between clinical complexity and high-alert medications20.
There is currently sufficient evidence to support the use of technologies related to medication administration for the benefit of patient safety; however, the process of implementing error reduction programs is not straightforward. Strategic planning, investment of time and money, standardization of medication and dosing practices by multidisciplinary teams (including pharmacists, specialized nurses, and physicians), development of drug libraries, training in the appropriate use of technology and library programming, adoption of the technology by nursing professionals, and the promotion of a safety culture related to medication administration are required. In addition, ongoing monitoring is necessary to allow for adjustments or the incorporation of new medications. Together, these requirements pose a challenge for institutions and health systems in terms of quality of care21-25.
Limitations: Those related to sample selection and potential failures in data reception arising from interoperability between smart infusion pumps and the monitoring platform (IQ Enterprise®). For the purposes of the study, only data from the first year of the drug library implementation were analyzed, focusing on compliance and errors related to high-alert medications in terms of dose programming
Conclusions
This study found a 66% compliance rate with the drug libraries integrated into smart infusion pumps across five adult ICUs during the first year of use. The configuration of hard limits contributed to reducing clinical practice errors involving high-alert medications such as midazolam, fentanyl, and noradrenaline.
The findings support the conclusion that the implementation of institutional monitoring programs for the safe medication administration, supported by technologies such as DERS integrated into smart infusion pumps, contributes to reducing errors in clinical practice, with a positive impact on patient safety, institutional continuous improvement processes, and the strengthening of the professional role of nursing.
Conflict of interest: The authors declare no conflicts of interest.
Funding: Authors’ own resources.
References
X
Referencias
Borrelli EP, Lucaci JD, Wilson NS, Taneja A, Weiss M, Beer I. Evaluating the Impact of Smart Infusion Pump Interoperability on Reducing Medication Administration Errors: A Systematic Literature Review. Med Devices (Auckl). 2025;18:247-60. https://doi.org/10.2147/MDER.S522534
X
Referencias
Giuliano KK, Mahuren RS, Balyeat J. Data-based program management of system-wide IV smart pump integration. American Journal of Health-System Pharmacy. 2024;81(1):e30-6. https://doi.org/10.1093/ajhp/zxad245
X
Referencias
Shah N, Jani Y. Implementation of Smart Infusion Pumps: A Scoping Review and Case Study Discussion of the Evidence of the Role of the Pharmacist. Pharmacy. 2020;8(4):239. https://doi.org/10.3390/pharmacy8040239
X
Referencias
Olson C, Bouchard C. Optimizing the Smart Pump Drug Library Update Process: An Ongoing Effort at an Academic Medical Center. Patient Safety. 2024;6(1). https://doi.org/10.33940/001c.123222
X
Referencias
Herrero L, Cano M, Ratwani R, Sánchez L, Sánchez B, Sancibrián R, et al. A review of human factors and infusion pumps: lessons for procurement. Front Digit Health. 2025;7:1425409. https://doi.org/10.3389/fdgth.2025.1425409
X
Referencias
Kuitunen S, Airaksinen M, Holmström AR. Evolution of Intravenous Medication Errors and Preventive Systemic Defenses in Hospital Settings—A Narrative Review of Recent Evidence. Journal of Patient Safety. 2024;20(4):e29-39. https://doi.org/10.1097/PTS.0000000000001222
X
Referencias
Schnock KO, Dykes PC, Albert J, Ariosto D, Call R, Cameron C, et al. The frequency of intravenous medication administration errors related to smart infusion pumps: a multihospital observational study. BMJ Quality & Safety. 2017;26(2):131-40. https://doi.org/10.1136/bmjqs-2015-004465
X
Referencias
Kuitunen S, Kärkkäinen K, Linden-Lahti C, Schepel L, Holmström AR. Dose error reduction software in medication safety risk management – optimising the smart infusion pump dosing limits in neonatal intensive care unit prior to implementation. BMC Pediatr. 2022;22(1):118. https://doi.org/10.1186/s12887-022-03183-8
X
Referencias
López-Romero LA, Cáceres Rivera DI, Dueñas Badillo RE, Acosta-Barón JV, Robles Méndez IY, Rincón Castillo D, et al. Adherencia y potenciales eventos adversos prevenidos durante la administración de medicamentos endovenosos empleando bombas de infusión inteligentes en cuatro unidades de cuidados intensivos en Colombia. Rev Univ Ind Santander Salud. 2019;51(4):289-300. https://doi.org/10.18273/revsal.v51n4-2019002
X
Referencias
Narváez-Martínez MA, Rosas-Santana A, Rojas-Castañeda YA, Zapata-Cristancho DC. Master Dataset: Monitoring smart infusion pumps in adult intensive care units. Mendeley Data. 2025. https://doi.org/10.17632/f2mdstz6xz.1
X
Referencias
Carrington-Hahn S, Gosselin T, Frasure III E, Reynolds SS. Smart pump technology and dose error reduction. American Nurse Journal. 2025;20(01):33-6. https://doi.org/10.51256/ANJ012533
X
Referencias
Sutherland A, Gerrard WS, Patel A, Randall M, Weston E. The impact of drug error reduction software on preventing harmful adverse drug events in England: a retrospective database study. BMJ Open Quality. 2022;11(3):1-9. https://doi.org/10.1136/bmjoq-2021-001708
X
Referencias
Skog J, Rafie S, Schnock KO, Yoon C, Lipsitz S, Lew P. The Impact of Smart Pump Interoperability on Errors in Intravenous Infusion Administrations: A Multihospital Before and After Study. Journal Patient Safety. 2022;18(3):e666-71. https://doi.org/10.1097/PTS.0000000000000905
X
Referencias
Ibarra-Pérez R, Puértolas-Balint F, Lozano-Cruz E, Zamora-Gómez SE, Castro-Pastrana LI. Intravenous Administration Errors Intercepted by Smart Infusion Technology in an Adult Intensive Care Unit. Journal Patient Safety. 2021;17(6):430-6. https://doi.org/10.1097/PTS.0000000000000374
X
Referencias
Gray J, Ruggia-Check C, Mentzer L, Finn J, Frezghi F, Riesen A, et al. 1247: Impact of implementation of smart pump interoperability and drug library optimization. Critical Care Medicine. 2024;52(1):S595-S595. . https://doi.org/10.1097/01.ccm.0001003152.59872.b4
X
Referencias
Chin K, Donovan J, Bingham G, Poole S, Tong E. Evaluation of Smart Pump Interoperability with an Electronic Medical Record System to Improve Infusion Safety. IOS Press; 2024:1341-1342. https://doi.org/10.3233/SHTI231185
X
Referencias
VanHorn T, Harris J, Mayes S, Infanti LM, Kennedy A. Evaluation of the Effect of Smart Pump Interoperability on Infusion Errors in the Pediatric Hospital Setting. J Pediatr Pharmacol Ther. 2024;29(3):323-30. https://doi.org/10.5863/1551-6776-29.3.323
-
Michalek C, Carson SL. Implementing barcode medication administration and smart infusion pumps is just the beginning of the safety journey to prevent administration errors. Farmcia Hosp. 2020;44(3):114-21. http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S1130-63432020000300008&lng=es
-
Vanderveen T, O’Neill S, Beard JW. How Can We Tell How “Smart” Our Infusion Pumps Are? Anesthesia Patient Safety Foundation. 2020;35(1):21-22. https://www.apsf.org/article/how-can-we-tell-how-smart-our-infusion-pumps-are/
-
Borrelli EP, Lucaci JD, Wilson NS, Taneja A, Weiss M, Beer I. Evaluating the Impact of Smart Infusion Pump Interoperability on Reducing Medication Administration Errors: A Systematic Literature Review. Med Devices (Auckl). 2025;18:247-60. https://doi.org/10.2147/MDER.S522534
-
Giuliano KK, Mahuren RS, Balyeat J. Data-based program management of system-wide IV smart pump integration. American Journal of Health-System Pharmacy. 2024;81(1):e30-6. https://doi.org/10.1093/ajhp/zxad245
-
Institute for Safe Medication Practices (ISMP). Guidelines for Optimizing Safe Implementation and Use of Smart Infusion Pumps. ISMP. [Internet] 2020 [Cited 2025 August 01]. Available from: https://home.ecri.org/blogs/ismp-resources/guidelines-for-optimizing-safe-implementation-and-use-of-smart-infusion-pumps
-
Joint Commission. Sentinel Event Alert 63: Optimizing smart infusion pump safety with DERS [Internet]. 2021. [Cited 2025 August 01]. Available from: https://www.jointcommission.org/en-us/knowledge-library/newsletters/sentinel-event-alert/issue-63
-
Shah N, Jani Y. Implementation of Smart Infusion Pumps: A Scoping Review and Case Study Discussion of the Evidence of the Role of the Pharmacist. Pharmacy. 2020;8(4):239. https://doi.org/10.3390/pharmacy8040239
-
Alamer F, Alanazi AT. The Impact of Smart Pump Technology in the Healthcare System: A Scope Review. Cureus. 2023;15(3):e36007. https://doi.org/10.7759/cureus.36007
-
Olson C, Bouchard C. Optimizing the Smart Pump Drug Library Update Process: An Ongoing Effort at an Academic Medical Center. Patient Safety. 2024;6(1). https://doi.org/10.33940/001c.123222
-
Herrero L, Cano M, Ratwani R, Sánchez L, Sánchez B, Sancibrián R, et al. A review of human factors and infusion pumps: lessons for procurement. Front Digit Health. 2025;7:1425409. https://doi.org/10.3389/fdgth.2025.1425409
-
Kuitunen S, Airaksinen M, Holmström AR. Evolution of Intravenous Medication Errors and Preventive Systemic Defenses in Hospital Settings—A Narrative Review of Recent Evidence. Journal of Patient Safety. 2024;20(4):e29-39. https://doi.org/10.1097/PTS.0000000000001222
-
Agency for Healthcare Research and Quality, Rockville, MD. Making Health Care Safer II: An Updated Critical Analysis of the Evidence for Patient Safety Practices. [Internet] 2023 [Cited 2025 August 01]. Available from: URL https://www.ahrq.gov/research/findings/evidence-based-reports/ptsafetyuptp.html
-
Schnock KO, Dykes PC, Albert J, Ariosto D, Call R, Cameron C, et al. The frequency of intravenous medication administration errors related to smart infusion pumps: a multihospital observational study. BMJ Quality & Safety. 2017;26(2):131-40. https://doi.org/10.1136/bmjqs-2015-004465
-
Kuitunen S, Kärkkäinen K, Linden-Lahti C, Schepel L, Holmström AR. Dose error reduction software in medication safety risk management – optimising the smart infusion pump dosing limits in neonatal intensive care unit prior to implementation. BMC Pediatr. 2022;22(1):118. https://doi.org/10.1186/s12887-022-03183-8
-
López-Romero LA, Cáceres Rivera DI, Dueñas Badillo RE, Acosta-Barón JV, Robles Méndez IY, Rincón Castillo D, et al. Adherencia y potenciales eventos adversos prevenidos durante la administración de medicamentos endovenosos empleando bombas de infusión inteligentes en cuatro unidades de cuidados intensivos en Colombia. Rev Univ Ind Santander Salud. 2019;51(4):289-300. https://doi.org/10.18273/revsal.v51n4-2019002
-
Narváez-Martínez MA, Rosas-Santana A, Rojas-Castañeda YA, Zapata-Cristancho DC. Master Dataset: Monitoring smart infusion pumps in adult intensive care units. Mendeley Data. 2025. https://doi.org/10.17632/f2mdstz6xz.1
-
Carrington-Hahn S, Gosselin T, Frasure III E, Reynolds SS. Smart pump technology and dose error reduction. American Nurse Journal. 2025;20(01):33-6. https://doi.org/10.51256/ANJ012533
-
Sutherland A, Gerrard WS, Patel A, Randall M, Weston E. The impact of drug error reduction software on preventing harmful adverse drug events in England: a retrospective database study. BMJ Open Quality. 2022;11(3):1-9. https://doi.org/10.1136/bmjoq-2021-001708
-
Skog J, Rafie S, Schnock KO, Yoon C, Lipsitz S, Lew P. The Impact of Smart Pump Interoperability on Errors in Intravenous Infusion Administrations: A Multihospital Before and After Study. Journal Patient Safety. 2022;18(3):e666-71. https://doi.org/10.1097/PTS.0000000000000905
-
Ibarra-Pérez R, Puértolas-Balint F, Lozano-Cruz E, Zamora-Gómez SE, Castro-Pastrana LI. Intravenous Administration Errors Intercepted by Smart Infusion Technology in an Adult Intensive Care Unit. Journal Patient Safety. 2021;17(6):430-6. https://doi.org/10.1097/PTS.0000000000000374
-
Heron C. Implementing smart infusion pumps with dose-error reduction software: real-world experiences. British Journal of Nursing. 2017;26(8):S13-6. https://doi.org/10.12968/bjon.2017.26.8.S13
-
Gray J, Ruggia-Check C, Mentzer L, Finn J, Frezghi F, Riesen A, et al. 1247: Impact of implementation of smart pump interoperability and drug library optimization. Critical Care Medicine. 2024;52(1):S595-S595. . https://doi.org/10.1097/01.ccm.0001003152.59872.b4
-
Chin K, Donovan J, Bingham G, Poole S, Tong E. Evaluation of Smart Pump Interoperability with an Electronic Medical Record System to Improve Infusion Safety. IOS Press; 2024:1341-1342. https://doi.org/10.3233/SHTI231185
-
Sowan A, Ha B. Maximizing the impact of smart pump-EHR interoperability in critical care. Intensive Crit Care Nurs. 2024;85:103809. . https://doi.org/10.1016/j.iccn.2024.103809
-
VanHorn T, Harris J, Mayes S, Infanti LM, Kennedy A. Evaluation of the Effect of Smart Pump Interoperability on Infusion Errors in the Pediatric Hospital Setting. J Pediatr Pharmacol Ther. 2024;29(3):323-30. https://doi.org/10.5863/1551-6776-29.3.323