Rev Cuid. 2026; 17(1): 5220
Abstract
Introduction: The deterioration of social determinants of health across the life course may act as a relevant factor in increasing the risk of frailty and falls, thereby exacerbating social and health problems. Objective: To analyze whether social disadvantages experienced during different stages of life are associated with the occurrence of falls among older adults. Materials and Methods: A prospective study was conducted based on the Seniors-ENRICA-1 cohort, including 2,501 Spanish participants aged 60 years or older. Falls and falls requiring medical attention were considered the study outcomes. Exposure was defined as the level of lifelong social disadvantage, assessed across childhood, youth, adulthood, and old age. Bivariate analyses and logistic regression models adjusted for sociodemographic, clinical, and lifestyle variables were applied. Results: Individuals with low educational attainment were 1.4 times more likely to experience a fall compared to those with higher education. Additionally, individuals without an occupation in adulthood had an 80% higher probability of falling. No significant associations were found with the father's occupation or with household conditions in old age. Discussion: There is agreement that falls in older adults are associated with accumulated social inequalities, especially low educational attainment and occupation. Variables such as age, lifestyle, and medication use also have an influence. The socioeconomic situation is analyzed from an alternative perspective. Conclusion: Accumulated disadvantages in education and occupation increase the risk of falls in older adults.
Keywords: Accidental Falls; Aged; Socioeconomic Disparities in Health; Occupations.
Resumen
Introducción: El deterioro de los determinantes sociales de la salud a lo largo del curso de vida puede incidir como factor relevante en el aumento del riesgo de fragilidad y caídas agravando los problemas sociales y sanitarios. Objetivo: Analizar si las desventajas sociales experimentadas durante distintas etapas de la vida se asocian con la ocurrencia de caídas en personas mayores. Materiales y Métodos: Estudio prospectivo basado en la cohorte ENRICA Senior I, con 2.501 participantes españoles de 60 años o más. Se consideraron como desenlaces las caídas y las caídas que requirieron atención médica; y como exposición, el nivel de desventaja social a lo largo de la vida, evaluado en infancia, juventud, adultez y vejez. Se aplicaron análisis bivariados y modelos de regresión logística ajustados por variables sociodemográficas, clínicas y de estilo de vida. Resultados: Las personas con nivel educativo bajo presentaron 1,4 veces más probabilidad de caerse respecto a quienes tenían estudios superiores; quienes no contaban con ocupación en la adultez mostraron un 80% más de probabilidad de caída. No se hallaron asociaciones significativas con la ocupación del padre ni con las condiciones del hogar en la vejez. Discusión: Hay concordancia en que las caídas en adultos mayores están asociadas a desigualdades sociales acumuladas, especialmente bajo nivel educativo y la ocupación, variables como edad, estilo de vida y consumo de medicamentos también influyen. La situación socioeconómica cuenta con una perspectiva alternativa de análisis. Conclusión: Desventajas acumuladas en educación y la ocupación incrementan el riesgo de caídas en adultos mayores.
Palabras Clave: Accidentes por Caídas; Anciano; Desventaja Social en Salud; Ocupaciones.
Resumo
Introdução: A deterioração dos determinantes sociais da saúde ao longo da vida pode contribuir significativamente para o aumento do risco de fragilidade e quedas, exacerbando problemas sociais e de saúde. Objetivo: Analisar se as desvantagens sociais vivenciadas em diferentes fases da vida estão associadas à ocorrência de quedas em idosos. Materiais e Métodos: Estudo prospectivo baseado na coorte ENRICA Senior I, com 2.501 participantes espanhóis com 60 anos ou mais. Os desfechos incluíram quedas e quedas que necessitaram de atendimento médico; a exposição foi definida como o nível de desvantagem social ao longo da vida, avaliado na infância, juventude, idade adulta e velhice. Foram aplicadas bivariadas e modelos de regressão logística ajustados para variáveis sociodemográficas, clínicas e de estilo de vida. Resultados: Indivíduos com baixa escolaridade apresentaram 1,4 vezes mais probabilidade de sofrer quedas do que aqueles com maior escolaridade; aqueles que estavam desempregados na idade adulta apresentaram uma probabilidade 80% maior de sofrer quedas. Não foram encontradas associações significativas com a ocupação do pai ou com as condições de moradia na velhice. Discussão: Há consenso de que as quedas em idosos estão associadas a desigualdades sociais acumuladas, especialmente baixa escolaridade e ocupação. Variáveis como idade, estilo de vida e uso de medicamentos também desempenham um papel importante. O status socioeconômico oferece uma perspectiva alternativa para análise. Conclusão: As desvantagens acumuladas na educação e na ocupação aumentam o risco de quedas em idosos.
Palavras-Chave: Acidentes por Quedas; Idoso; Disparidades Socioeconômicas em Saúde; Ocupações.
Introduction
Falls are the second leading cause of death from accidental injuries, representing a major global public health problem1. Older adults aged 65 years and older are the most affected population2,3. Ten years ago in the United States, older adults experienced multiple falls each year requiring medical attention, negatively affecting healthcare costs estimated at 28 billion US dollars annually3, which are projected to triple due to the growth of this population. However, in Brazil, primary health care annually contributes to reducing the costs associated with falls among older adults, due to the existence of programs such as home health care, which contribute to shortening hospital stays4. In Spain, 30% of adults aged 65 years and older experience falls, and half will experience a subsequent fall in the coming months5,6. These falls will increase over time, with variations in their prevalence associated with functional decline and social and economic conditions.
Similarly, among older adults, the occurrence of falls may be influenced by favorable or unfavorable social and environmental conditions in which they live. These living conditions constitute the theoretical construct and reference known as the social determinants of health, as defined by the World Health Organization, and may have cumulative and differential effects across the life course7. This may or may not constitute an advantage in facing the challenges associated with aging8. However, the lack of age-appropriate housing conditions and social isolation are considered social disadvantages that increase the risk of falls, and that such an event could result in hospitalization9. The differences that exist between socioeconomic levels have a differential impact on some of these groups, increasing the risk of physical disability, frailty, and falls, with their respective social consequences8,10.
Recently, in France and Sweden, the relationship between falls and multiple factors, including age, frailty, and living environment, was analyzed. Social disadvantages within these social determinants of health have been recently addressed, showing how they negatively interact with dependency among older adults and, collectively, with chronic diseases11-13. Lifelong social disadvantages and other age-related factors, such as hospitalization in palliative care units14, increase the risk of frailty, the risk of falls, and the risk of mortality14,15, which in 2021 reached a rate of 78 per 100,000 inhabitants16. In high-income countries, this situation accounts for between 0.8% and 1.5% of total annual healthcare costs12,17.
In particular, socially disadvantaged groups due to financial, educational, and employment difficulties are more likely to report frailty and poor health, which could be reversed by improving the living conditions of this population12. In this context, social disadvantages in old age are associated with the current social and environmental conditions of the household in which older adults reside and are identified as an important social determinant of health.
The objective of this study was to analyze the influence of lifelong social disadvantages and their association with falls among older adults in Spain.
Materials and Methods
Study design
This cohort study was conducted among adults evaluated in the Seniors Study on Nutrition and Cardiovascular Risk in Spain (ENRICA) 118-20. EThe Seniors-ENRICA-1 study was initiated in Madrid, Spain, with a baseline conducted in 2008 among men and women aged 60 and older who were invited to participate voluntarily, and who were followed up on two occasions: 1) 2012-2013 and 2) 2014-2015. The study participants were representative of the Spanish population and were selected using a multi- stage stratified cluster sampling approach. Within each stratum, households were randomly selected, first according to province and municipality size. Households were then selected through telephone dialing, using the telephone directory as the sampling frame. It was possible to estimate prevalence rates with a sampling error of less than 3% and a confidence level of 95%. Likewise, the sample size allowed the detection of associations with relative risks ranging from 1.3 to 1.5, which are considered epidemiologically and clinically relevant.
Households were selected proportionally by sex and age, and sociodemographic data were subsequently collected by telephone. During an in-person visit, blood and urine samples were collected, and physical examinations and dietary-habit interviews were conducted. Overall, the study achieved an above-average response rate of 51%. This figure is comparable to that of other large- scale population studies, which are not free from potential selection bias. However, the stratified random sampling design, together with the application of weighting factors for age, sex, and region, improved the representativeness of the sample and mitigated these limitations.
Participants who had died (n=95) were excluded from the first follow-up in 2012-2013, as were those with evidence of cognitive impairment for whom proxy information (n=18) could not be obtained from their relatives or caregivers. Of the original sample of 2,614 participants19, 2,501 older adults formed the final sample and were included in the data analysis.
All study participants provided written informed consent before the assessment began. The study was approved by the clinical research ethics committees of La Paz University Hospital in Madrid and Hospital Clinic in Barcelona19.
Variables and assessment instruments
Falls: These are defined as an involuntary loss of balance and support, which inadvertently causes a person to fall to the ground or to a lower level than where they were. This variable was assessed dichotomously (yes/no) and included in the Seniors-ENRICA-1 study19.
Falls requiring medical attention: For this category, all events following a fall that resulted in a visit to a physician, attendance at an emergency department, or hospitalization were considered. This variable was measured dichotomously (fall without medical attention/fall with medical attention) and included in the Seniors-ENRICA-1 study19.
Lifelong social disadvantage among older people: This variable is understood as the combination of different circumstances experienced over the years21-23. Social disadvantage was assessed across life stages, including childhood, youth, adulthood, and old age; therefore, it was considered that the accumulation of deprivations across these four stages could define lifelong social disadvantage, this variable was measured dichotomously (yes/no) according to whether these characteristics were present Table 1.
Table 1. Lifelong social disadvantages throughout the life course: definition
X
Table 1. Lifelong social disadvantages throughout the life course: definition
| Stage of life |
Social disadvantage indicator |
Description |
| Childhood |
Father’s occupation |
Initial socioeconomic conditions of the household; manual labor24 or unskilled occupations. |
| Youth |
Educational level attained |
The absence of higher education or completion of only primary/secondary education. |
| Adulthood |
Own occupation |
Employment in unskilled, informal jobs or the absence of formal employment. |
| Old age |
Current household conditions |
Lack of home ownership, insufficient material resources, or inadequate living conditions. |
Sociodemographic and lifestyle variables: The following variables were recorded: sex, age, smoking status (never smoker, former smoker, current smoker), alcohol intake (g/day) and/or former drinker (yes/no), adherence to Mediterranean diet (yes/no), dietary calcium intake (continuous), vitamin D intake (continuous), caffeine intake (continuous), physical activity (continuous; leisure time + at home), hours of TV/week (continuous), hours of sleep (continuous; nighttime + daytime), overall obesity (yes/no), abdominal obesity (yes/no), hypertension (yes/no), diabetes (yes/no), cardiovascular disease (yes/no), number of other prevalent diseases (continuous), number of medications (continuous; Medications - 1), use of sleeping pills (yes/no), and history of fracture (yes/ no). These other considerations were taken into account to construct a model aimed at explaining the occurrence of the falls outcome under study.
Data analysis
Multinomial logistic regression analysis was conducted using Stata (version 12.0; StataCorp., College Station, Texas, United States). Data distribution normality was assessed using the Shapiro-Wilk test. For quantitative variables, independent-samples t-tests were performed, whereas chi-square tests were used for categorical variables. Odds ratios (ORs) for the risk of falls were estimated for lifelong socioeconomic status, along with their corresponding 95% confidence intervals (95% CI). All p-values < 0.05 were considered statistically significant.
The variables “falls” and “falls requiring medical attention” were analyzed in association with lifelong social disadvantages. Additional analyses were conducted for each variable, including father's occupation, participants' occupation, educational level, and current household disadvantage. Each of these analyses was adjusted for secondary independent variables (confounders) and fitted using three models: Model 1, adjusted for sex and age (continued); model 2, which included model 1 + smoking status (never smoker, former smoker, current smoker), alcohol intake (g/day) and/or former drinker (yes/ no), adherence to Mediterranean diet (yes/no), dietary calcium intake (continuous), vitamin D intake (continuous), caffeine intake (continuous), physical activity (continuous; leisure time + at home), hours of TV/week (continuous), hours of sleep (continuous; nighttime + daytime), overall obesity (yes/no), abdominal obesity (yes/no); and model 3, which included model 2 + hypertension (yes/no), diabetes (yes/no), cardiovascular disease (yes/no), number of other prevalent diseases (continuous), number of medications (continuous; Medications - 1), and use of sleeping pills (yes/no). All collected data is freely available for access and consultation in Mendeley Data25.
Results
Table 2 presents the sociodemographic characteristics, lifestyles, and presence of chronic diseases among older adults evaluated in the Seniors-ENRICA-1 study, according to whether they reported having experienced a fall or not. Additionally, these characteristics are reported for older adults who experienced a fall, distinguishing between those who did not require medical attention and those who did. Significant differences were observed between older adults who reported having experienced a fall and those who reported no falls, and between those who experienced a fall with and without medical attention, in relation to age, tobacco use, alcohol consumption, adherence to the Mediterranean diet, physical activity, presence of cardiovascular disease, and medication use.
Table 2. Characteristics of the older adult population in Spain according to the incidence of falls and falls requiring medical attention. n=2501
X
Table 2. Characteristics of the older adult population in Spain according to the incidence of falls and falls requiring medical attention. n=2501
| Sociodemographic and lifestyle variables |
No falls (n=1969) %(n) |
Falls (n=532) %(n) |
p-value |
Falls without medical attention (n=292) %(n) |
Falls with medical attention (n=240) %(n) |
p-value |
| Sex |
|
|
|
|
|
< 0.001* |
| Men |
51.60 (1016) |
29.70 (158) |
< 0.001* |
36.99 (108) |
20.83 (50) |
|
| Age. years. Mean ± SD |
68.32 ± 6.20 |
69.91 ± 6.80 |
< 0.001* |
69.23 ± 6.55 |
70.75 ± 7.02 |
0.010* |
| Tobacco use |
|
|
|
|
|
0.320 |
| Never smoked |
55.97 (1102) |
69.17 (368) |
|
66.78 (195) |
72.08 (173) |
|
| Former smoker |
32.00 (630) |
22.56 (120) |
<0.001* |
25.00 (73) |
19.58 (47) |
|
| Current smoker |
12.04 (237) |
8.27 (44) |
|
8.22 (24) |
8.33 (20) |
|
| Alcohol consumption |
|
|
|
|
|
0.110 |
| Never a drinker |
24.33 (479) |
35.15 (187) |
|
31.16 (91) |
40.00 (96) |
|
| Former drinker |
9.60 (189) |
10.53 (56) |
<0.001* |
9.93 (29) |
11.25 (27) |
|
| Moderate consumption |
18.33 (361) |
19.92 (106) |
|
20.89 (61) |
18.75 (45) |
|
| Excessive consumption |
47.74 (940) |
34.40 (183) |
|
38.01 (111) |
30.00 (72) |
|
| Adherence to the Mediterranean diet |
24.94 (491) |
19.74 (105) |
0.013* |
23.29 (68) |
15.42% (37) |
0.020* |
| Dietary calcium intake. Mean ± SD |
890.62 ± 355.74 |
877.46 ± 330.38 |
0.440 |
898.53 ± 340.31 |
851.84±316.71 |
0.100 |
| Vitamin D intake. Mean ± SD |
3.47 ± 3.17 |
3.25 ± 2.86 |
0.140 |
3.42 ± 2.84 |
3.04±2.87 |
0.130 |
| Caffeine intake. Mean ± SD |
72.50 ± 108.70 |
66.59 ± 124.68 |
0.280 |
71.38 ± 145.51 |
60.77±93.27 |
0.320 |
| Leisure-time PA. MET– h/week. Mean ± SD |
22.43 ± 15.57 |
19.32 ± 13.96 |
<0.001* |
19.42 ± 14.16 |
19.19±13.75 |
0.850 |
| PA at home. MET– h/week. mean ± SD |
36.39 ± 32.06 |
42.36 ± 33.03 |
<0.001* |
40.18 ± 32.21 |
45.01±33.89 |
0.090* |
| Hours of TV per week. Mean ± SD |
17.52 ± 10.62 |
20.12 ± 13.29 |
<0.001* |
19.35 ± 13.12 |
21.05±13.47 |
0.140 |
| Hours of nighttime sleep. Mean ± SD |
6.89 ± 1.35 |
6.73 ± 1.52 |
0.010* |
6.72 ± 1.41 |
6.75±1.64 |
0.780 |
| Hours of daytime sleep. Mean ± SD |
0.29 ± 0.55 |
0.26 ± 0.49 |
0.240 |
0.28 ± 0.50 |
0.23±0.48 |
0.270 |
| Overall obesity |
|
|
|
|
|
|
| Less than 25 |
20.06 (395) |
22.18 (118) |
|
20.21 (59) |
0 (0) |
2.540 |
| Between 25 and 30 |
49.06 (966) |
45.49 (242) |
0.316 |
44.86 (131) |
0.28 (1) |
2.540 |
| More than 30 |
30.88 (608) |
32.33 (172) |
|
34.93 (102) |
0 (0) |
2.540 |
| Abdominal obesity |
56.58 (1114) |
60.53 (322) |
0.100 |
58.56 (171) |
62.92 (151) |
0.300 |
| Hypertension |
63.59 (1252) |
66.17 (352) |
0.270 |
66.78 (195) |
65.42 (157) |
0.740 |
| Diabetes |
15.64 (308) |
15.23 (81) |
0.810 |
15.75 (46) |
14.58 (35) |
0.700 |
| CV disease |
2.04 (40) |
3.89 (21) |
0.020* |
93.08 (272) |
11.4 (27) |
0.360 |
| No. of other prevalent diseases. Mean ± SD |
1.64 ± 1.16 |
2.08 ± 1.34 |
<0.001* |
1.94 ± 1.32 |
2.25 ± 1.33 |
0.009* |
| No. of medications. Mean ± SD |
1.90 ± 1.88 |
2.31 ± 2.14 |
<0.001* |
2.20 ± 2.08 |
2.44 ± 2.21 |
0.200 |
| Use of sleeping pills |
|
|
|
|
|
|
| No |
82.17 (1618) |
70.86 (377) |
|
75.68 (221) |
65.00 (156) |
|
| Sometimes |
5.89 (116) |
6.39 (34) |
<0.001* |
6.85 (20) |
5.83 (14) |
0.015* |
| Usually |
11.93 (235) |
22.74 (121) |
|
17.47 (51) |
29.17 (70) |
|
PA=Physical activity, CV=Cardiovascular, h=hours, SD=Standard deviation, MET= metabolic equivalent of task (energy cost of a person at rest). No.=Number. For quantitative variables, independent-samples t-tests were performed, and for categorical variables, a chi-square tests were used. *Statistically significant differences were considered at p<0.05.
No differences were observed in lifelong social disadvantages between older adults who reported having experienced a fall and those who reported no falls, nor between those who experienced a fall with or without medical attention Table 3.
Table 3. Lifelong social disadvantage of older adults according to fall risk. n=2,501.
X
Table 3. Lifelong social disadvantage of older adults according to fall risk. n=2,501.
| Lifelong social disad- vantage of older adults |
No falls (n=1969) %(n) |
With falls (n=532 ) %(n) |
p-value |
Falls without medical attention (n=292) %(n) |
Falls with medical attention (n=240) %(n) |
p-value |
| Disadvantage in child-hood |
|
|
|
|
|
0.380 |
| Father's occupation: manual labor |
33.01 (650) |
31.39 (167) |
0.470 |
29.79 (87) |
33.33 (80) |
|
| Disadvantage in youth: Level of education |
|
|
|
|
|
0.110 |
| Primary education |
53.89 (1061) |
56.95 (303) |
|
53.08 (155) |
61.67 (148) |
|
| Secondary education |
24.53 (483) |
23.68 (126) |
0.400 |
25.00 (73) |
22.08 (53) |
|
| University education |
21.58 (425) |
19.36 (103) |
|
21.92 (64) |
16.25 (39) |
|
| Disadvantage in adulthood |
|
|
|
|
|
0.340 |
| Own occupation: manual labor |
28.34 (558) |
34.21 (182) |
0.008 |
35.96 (105) |
32.08 (77) |
|
| Disadvantage in old age - Current household conditions |
|
|
|
|
|
0.610 |
| At least one |
83.44 (1643) |
85.15 (453) |
0.340 |
82.53 (241) |
89.33 (214) |
|
| Lifelong social disadvantage |
|
|
|
|
|
0.670 |
| All |
30.27 (596) |
27.63 (147) |
0.620 |
31.16 (91) |
23.33 (56) |
|
| Continuing lifelong social disadvantage. Mean ± SD |
2.17 ± 0.72 |
2.15 ± 0.72 |
0.560 |
2.12 ± 0.73 |
2.18 ± 0.72 |
0.340 |
For quantitative variables, independent-samples t-tests were performed, and for categorical variables, a chi-square tests were used. * Statistically significant differences were considered at p<0.05.
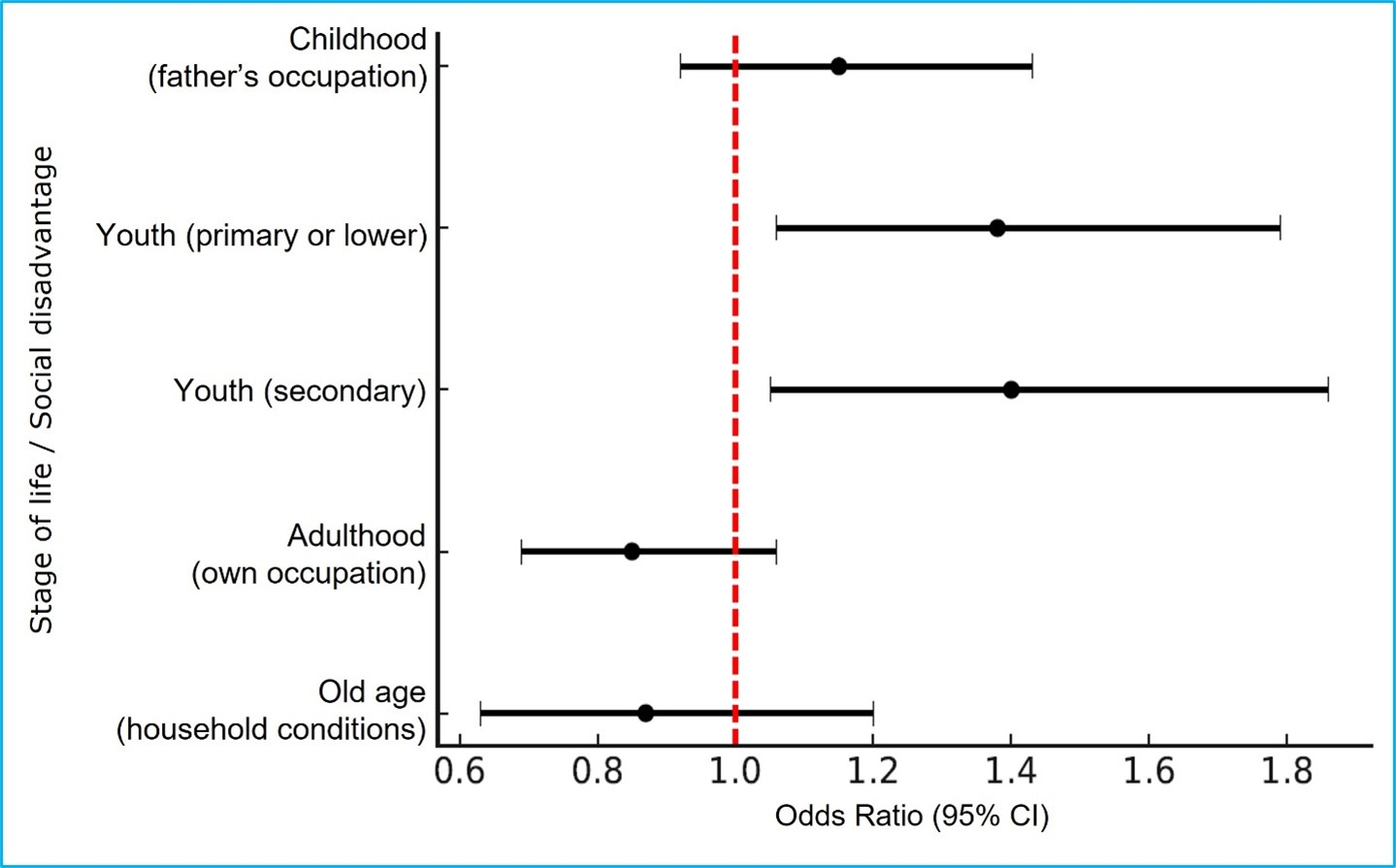
Table 4 and Figure 1 show the association between lifelong social disadvantage and falls among older adults. In the model adjusted for sociodemographic characteristics, lifestyles, and the presence of chronic diseases (Model 3), older adults with primary or lower education and those with secondary education had a 1.4-fold higher likelihood of experiencing a fall than those with higher education.
Furthermore, in the model adjusted for sex and age, older adults without an occupation in adulthood had an 80% higher likelihood of experiencing a fall compared with those who had their own occupation. Regarding social disadvantages assessed in childhood (father's occupation) and in old age (current household conditions), no significant associations were observed.
Table 4. Association between lifelong social disadvantage and falls in older adults in Spain
X
Table 4. Association between lifelong social disadvantage and falls in older adults in Spain
| Variables |
Model 1 |
p-value |
Model 2 |
p-value |
Model 3 |
p-value |
| OR ( 95% CI) |
|
OR ( 95% CI) |
|
OR ( 95% CI) |
|
| Childhood (Father's occupation) |
|
|
|
|
|
|
| Without disadvantage |
1 |
|
1 |
|
1 |
|
| Disadvantage |
1.05 (0.85-1.30) |
0.639 |
1.08 (0.87-1.34) |
0.467 |
1.15 (0.92-1.43) |
0.216 |
| Youth (Own level of education) |
|
|
|
|
|
|
| Higher Education |
1 |
|
1 |
|
1 |
|
| Primary or lower education |
1.15 (0.90-1.47) |
0.261 |
1.27 (0.99-1.64) |
0.062 |
1.38 (1.06-1.79) |
0.015* |
| Secondary education |
1.13 (0.87-1.47) |
0.351 |
1.32 (1.00-1.74) |
0.053 |
1.40 (1.05-1.86) |
0.022* |
| Adulthood (Own occupation) |
|
|
|
|
|
|
| Without disadvantage |
1 |
|
1 |
|
1 |
|
| Disadvantage |
0.80 (0.63-0.96) |
0.019* |
0.82 (0.66-1.01) |
0.063 |
0.85 (0.69-1.06) |
0.159 |
| Old age (Current household conditions) |
|
|
|
|
|
|
| Without disadvantage |
1 |
|
1 |
|
1 |
|
| Disadvantage |
0.98 (0.72-1.34) |
0.903 |
0.90 (0.65-1.24) |
0.512 |
0.87 (0.63-1.20) |
0.385 |
Multinomial logistic regression analysis was performed. Odds ratios (ORs) of falls in relation to lifelong socioeconomic status were estimated, along with their corresponding 95% confidence intervals (95% CI). Model 1: adjusted for sex and age (continuous). Model 2: Additionally adjusted for smoking status (never smoker, former smoker, current smoker), alcohol intake (never drinker, former drinker, moderate alcohol intake, excessive alcohol intake), adherence to Mediterranean diet (yes/no), dietary calcium intake (continuous), vitamin D intake (continuous), caffeine intake (continuous), leisure-time physical activity (continuous), physical activity at home (continuous), hours of TV/ week (continuous), hours of nighttime sleep (continuous), hours of daytime sleep (continuous), overall obesity (yes/no), abdominal obesity (yes/no). Model 3: additionally adjusted for hypertension (yes/no), diabetes (yes/no), cardiovascular disease (yes/no), number of other prevalent diseases (continuous), number of medications (continuous), and use of sleeping pills (yes/no). *p<0,05
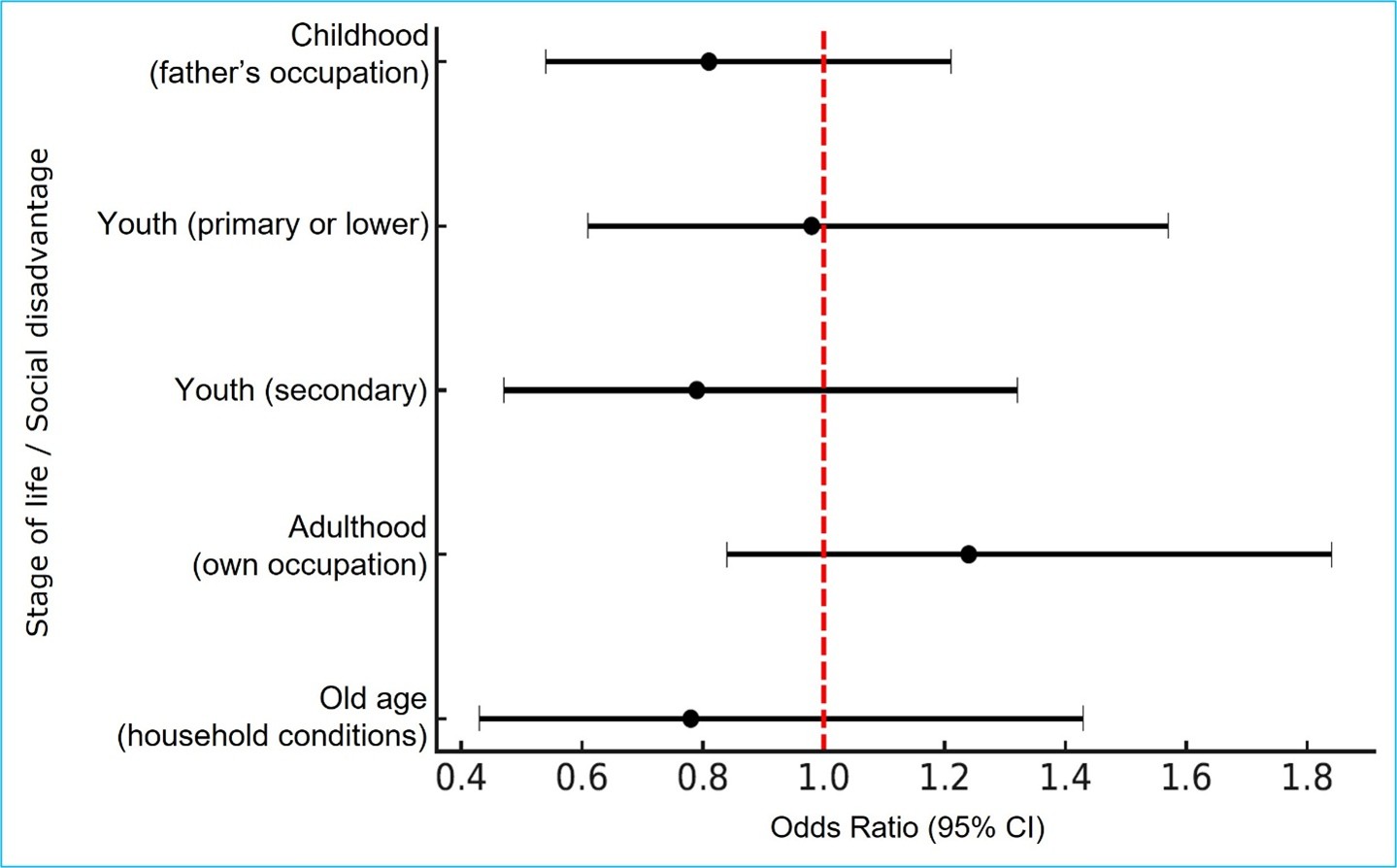
Additionally, no significant association was observed between lifelong social disadvantage and falls requiring medical attention Table 5 and Figure 2.
Table 5. Association between lifelong social disadvantage and falls requiring medical attention in older adults in Spain
X
Table 5. Association between lifelong social disadvantage and falls requiring medical attention in older adults in Spain
| Variables |
Model 1 |
p-value |
Model 2 |
p-value |
Model 3 |
p-value |
| OR ( 95% CI) |
|
OR ( 95% CI) |
|
OR ( 95% CI) |
|
| Childhood (Father's occupation) |
|
|
|
|
|
|
| Without disadvantage |
1 |
|
1 |
|
1 |
|
| Disadvantage |
0.80 (0.55-1.17) |
0.244 |
0.78 (0.53-1.16) |
0.222 |
0.81 (0.54-1.21) |
0.305 |
| Youth (Own level of education) |
|
|
|
|
|
|
| Higher Education |
1 |
|
1 |
|
1 |
|
| Primary or lower education |
0.92 (0.60-1.43) |
0.726 |
0.78 (0.60-1.50) |
0.808 |
0.98 (0.61-1.57) |
0.934 |
| Secondary education |
0.84 (0.52-1.36) |
0.477 |
0.78 (0.47-1.30) |
0.334 |
0.79 (0.47-1.32) |
0.368 |
| Adulthood (Own occupation) |
|
|
|
|
|
|
| Without disadvantage |
1 |
|
1 |
|
1 |
|
| Disadvantage |
1.29 (0.88-1.86) |
0.192 |
1.21 (0.82-1.77) |
0.339 |
1.24 (0.84-1.84) |
0.284 |
| Old age (Current household conditions) |
|
|
|
|
|
|
| Without disadvantage |
1 |
|
1 |
|
1 |
|
| Disadvantage |
0.82 (0.47-1.42) |
0.471 |
0.86 (0.48-1.52) |
0.600 |
0.78 (0.43-1.43) |
0.431 |
Odds ratios (ORs) for falls in relation to lifelong socioeconomic status were estimated, along with their corresponding 95% confidence inter-vals (95% CI). Model 1: adjusted for sex and age (continuous). Model 2: Additionally adjusted for smoking status (never smoker, former smoker, current smoker), alcohol intake (never drinker, former drinker, moderate alcohol intake, excessive alcohol intake), adherence to Mediterranean diet (yes/no), dietary calcium intake (continuous), vitamin D intake (continuous), caffeine intake (continuous), leisure-time physical activity (continuous), physical activity at home (continuous), hours of TV/week (continuous), hours of nighttime sleep (continuous), hours of daytime sleep (continuous), overall obesity (yes/no), abdominal obesity (yes/no). Model 3: additionally adjusted for hypertension (yes/no), diabetes (yes/ no), cardiovascular disease (yes/no), number of other prevalent diseases (continuous), number of medications (continuous), and use of sleeping pills (yes/no). *p<0,05.
Discussion
The results of this study reveal inequalities in falls among older adults in Spain. A higher probability of falls was observed among older adults with lower levels of education and without their own occupation.
Being female, older age, and behavioral factors such as watching television increase the risk of falls. Additionally, biological factors such as lifestyle, diabetes, and prevalent diseases, as well as the number of medications taken and the use of sleeping pills, were associated with falls in this study. No clear association was observed for socioeconomic status, specifically within categories that included occupation type.
It has been shown that lifelong socioeconomic inequalities affect health capital in old age. Regardless of how these inequalities are measured, the outcome is the same. Our study presents socioeconomic levels estimated across four life periods, in a manner similar to that described by Herr et al.12 However, in our study, childhood socioeconomic status was characterized based on the father's occupation, whereas in the French study, living standards were considered for this criterion. Furthermore, those researchers assessed the financial situation as an indicator of socioeconomic position in the most advanced stage of life, whereas in our study, household conditions were used for this phase.
Deprivation estimates reported in the studies by Khow et al.26 and Enderlin et al.27 qassociate the risk of falls in older adults with poor lighting, slippery surfaces, clutter, rugs, lack of ramps, lack of seat-lift devices, and lack of handrails. These findings are consistent with the deprivation analysis in our study, which identified conditions such as lack of heating, reporting feeling cold, and absence of an elevator.
Our study shows that economic, social, occupational, and educational conditions accumulated throughout life influence the risk of falls in older adults. Factors such as access to quality education and dignified work function as protective factors, whereas individuals who experience structural disadvantages in these areas are influenced by the economic and political models of each territory. In line with Lander, these inequalities are situated within a civilizational crisis in which capital, by prioritizing individual profit and corporate interests, deepens social and ecological asymmetries, thereby weakening solidarity and democracy. This highlights the need to engage in discussions on public social protection policies that recognize the impact of these demographic and social changes, adapt to population aging, and promote dignified, equitable, and solidarity-based aging in the context of a system that transfers the burden of care to families28.
Our results show an association between falls and increasing age. This result is consistent with those reported by Morrison et al.29, who indicate that the increased risk of falls is associated with a decline in physiological processes related to balance and gait. According to studies by Mata et al30. low levels of education are associated with frailty and falls. These results are consistent with our results, in which these outcomes were less frequent among participants with university-level or higher education low levels of education are associated with frailty and falls. These results are consistent with our results, in which these outcomes were less frequent among participants with university-level or higher education.
Furthermore, in our study, the use of sleeping pills, considered as a secondary independent variable, was associated with falls among older adults in Spain. Similarly, independent studies conducted in different settings by Martinez et al.31, como también por el grupo de Seitz et al.32 and by Diaz et al.33 have reported the same result.
This research provides a systematic assessment of the association between the level of social disadvantage, specifically in relation to household conditions, and falls, showing that the risk of falls increases as the level of education decreases.
Our research did not include institutionalized subjects, a circumstance in which adults are more prone to falling; therefore, the risk in this population group is underestimated. As in other population-based surveys, selection bias may be present, as approximately 25% of participants did not take part in the follow-up; consequently, information from these participants was not included in this study in order to address this situation.
One implication of our results is the need for government involvement in the implementation of interventions aimed at reducing the incidence of falls. Governments can promote public policies related to the design and construction of neighborhoods whose standards and conditions enable older adults to maintain mobility, through age-friendly urban design,34 cand through housing and environments equipped with devices to support older adults with mobility limitations.
A response rate of 51% may represent a limitation of this study. Although this value is comparable to that reported in other large population-based studies, it does not preclude the presence of potential selection bias. Therefore, the use of a stratified random sampling design strengthened the representativeness of the sample by applying weighting factors for age, sex, and region, thereby mitigating this limitation. Additionally, another limitation was that, although the study focuses on the general population of non-institutionalized older adults, individuals with severe cognitive impairment, serious communication difficulties, or conditions that prevented participation in the interview were excluded. This exclusion may have introduced selection bias, as older adults with greater social and clinical vulnerability were left out.
Conclusions
This study analyzed the association between social disadvantages and falls among older adults in Spain from a multifactorial relationship35, It should be emphasized that these conditions of inequality act as factors that contribute to and increase the risk of falls. Among the social disadvantages analyzed, not all showed significant associations; however, among those with the strongest associations, educational level and individuals’ own occupation were identified. Given that falls involve a set of interacting dimensions, this study presents a challenge to continue analyzing other factors that, although not statistically significant, such as social disadvantage in childhood and old age, may also contribute to fall incidents. For this reason, identifying these factors is relevant for proposing strategies to mitigate fall risk factors to prevent these outcomes among older adults36,37.
Conflict of interest: The authors declare no conflict of interest related to the review and analysis of the Seniors-ENRICA-I database.
Funding: This study received no funding from any institution.
Acknowledgments: The authors thank the Universidad Autónoma de Madrid and the Universidad del Norte for facilitating this research
References
X
Referencias
Pfortmueller CA, Lindner G, Exadaktylos AK. Reducing fall risk in the elderly: risk factors and fall prevention, a systematic review. Minerva Med. 2014;105(4):275-81. https://pubmed.ncbi.nlm.nih.gov/24867188/
X
Referencias
Pinheiro A, Schmidt AM, Simon C, Moura CMAB, Guerra D, Klipel GDS, et al. Economic overview of falls among elderly Brazilians. Epidemiologia e Servicos de Saude. Ministry of Health; 2022;31(2):e2022536. https://doi.org/10.1590/S2237-96222022000200024
X
Referencias
Lavedán Santamaría A, Jürschik Giménez P, Botigué Satorra T, Nuin Orrio C, Viladrosa Montoy M. Prevalencia y factores asociados a caídas en adultos mayores que viven en la comunidad. Aten Primaria. 2015;47(6):367–375. https://doi.org/10.1016/j.aprim.2014.07.012
X
Referencias
Organización Mundial de la Salud. Subsanar las desigualdades en una generación: Alcanzar la equidad sanitaria actuando sobre los determinantes sociales de la salud: resumen analítico del informe final. Consulta: Agosto 27, 2008. Disponible en: https://www.who.int/es/publications/i/item/WHO-IER-CSDH-08.1
X
Referencias
Garin N, Olaya B, Perales J, Moneta MV, Miret M, Ayuso-Mateos JL, et al. Multimorbidity patterns in a national representative sample of the Spanish adult population. PLoS One. 2014;9(1):e0123037. https://doi.org/10.1371/journal.pone.0084794
X
Referencias
Milos V, Bondesson Å, Magnusson M, Jakobsson U, Westerlund T, Midlöv P. Fall risk-increasing drugs and falls: a cross-sectional study among elderly patients in primary care. BMC Geriatric. 2014;40:14. https://doi.org/10.1186/1471-2318-14-40
X
Referencias
Herr M, Robine JM, Aegerter P, Arvieu JJ, Ankri J. Contribution of socioeconomic position over life to frailty differences in old age: comparison of life-course models in a French sample of 2350 old people. Ann Epidemiol. 2015;25(9):674-680. https://doi.org/10.1016/j.annepidem.2015.05.006
X
Referencias
Otani H, Shimoinaba J, Kashiwagi H, Morita T, Maeda I, Yokomichi N, et al. Prevalence of falls in the last weeks of life and relationship between falls, independence and quality of dying in Japan: a large prospective cohort study. BMJ Open. 2024;14:e085315. https://doi.org/10.1136/bmjopen-2024-085315
X
Referencias
De Vries OJ, Peeters GMEE, Lips P, Deeg DJH. Does frailty predict increased risk of falls and fractures? A prospective population-based study. Osteoporos Int. 2013;24:2397-2403. https://doi.org/10.1007/s00198-013-2303-z
X
Referencias
Nakanishi N, Nakura I, Nagano K, Yoneda H, Takatorige T, Shinsho F, et al. Mortality in Relation to The Type of Household Among Elderly People Living in a Community. Journal of Epidemiology. 1998;8(1):65-72. https://doi.org/10.2188/jea.8.65
X
Referencias
Guallar-Castillón P, Gil-Montero M, León-Muñoz LM, Graciani A, Bayán-Bravo A, Taboada JM, et al. Magnitude and management of hypercholesterolemia in the adult population of Spain, 2008- 2010: The ENRICA study. Rev Esp Cardiol. 2012;65(6):551–8. https://doi.org/10.1016/j.rec.2012.03.001
X
Referencias
Rodríguez-Artalejo F, Graciani A, Guallar-Castillón P, León-Muñoz LM, Zuluaga MC, López-García E, et al. Justificación y métodos del estudio sobre nutrición y riesgo cardiovascular en España (ENRICA). Rev Esp Cardiol. 2011;64(10):876–82. https://doi.org/10.1016/j.recesp.2011.05.019
X
Referencias
Zuluaga MC, Guallar-Castillón P, Conthe P, Rodríguez-Pascual C, Graciani A, León-Muñoz LM, et al. Housing conditions and mortality in older patients hospitalized for heart failure. American Heart Journal. 2011;161(5):950–5. https://doi.org/10.1016/j.ahj.2011.03.002
X
Referencias
McMunn A, Nazroo J, Breeze E. Inequalities in health at older ages: a longitudinal investigation of the onset of illness and survival effects in England. Age and Ageing. 2009;38(2):181-187.https://doi.org/10.1093/ageing/afn236
X
Referencias
Aromaa A, Koponen P, Tafforeau J, Vermeire C. Evaluation of Health Interview Surveys and Health Examination Surveys in the European Union. European Journal of Public Health. 2003;13(1):67-72. https://doi.org/10.1093/eurpub/13.suppl_1.67
X
Referencias
Instituto Nacional de Estadística. Clasificación nacional de ocupaciones 2011. Consulta: Noviembre 11, 2010.
X
Referencias
Salcedo Salgado JD. Data Base Enrica Senior I. Mendeley V1. 2025.
X
Referencias
Enderlin C, Rooker J, Ball S, Hippensteel D, Alderman J, Fisher SJ, et al. Summary of factors contributing to falls in older adults and nursing implications. Geriatr Nurs. 2015 ;36(5):397–406. https://doi.org/10.1016/j.gerinurse.2015.08.006
X
Referencias
Morrison S, Colberg SR, Parson HK, Neumann S, Handel R, Vinik EJ, et al. Walking-Induced Fatigue Leads to Increased Falls Risk in Older Adults. J Am Med Dir Assoc. 2016;17(5):402–409. https://doi.org/10.1016/j.jamda.2015.12.013
X
Referencias
Martinez-Cengotitabengoa M, Diaz-Gutierrez MJ, Besga A, Bermúdez-Ampudia C, López P, Rondon MB, et al. Benzodiazepine prescriptions and falls in older men and women. Revista de Psiquiatría y Salud Mental. 2018;11(1):12–8. https://doi.org/10.1016/j.rpsm.2017.01.004
X
Referencias
Seitz D, Iaboni A, Kirkham J. Psychotropic Drugs and Falls in Older Adults: an Update for the Geriatric Psychiatrist. The American Journal of Geriatric Psychiatry. 2017;25(3). https://doi.org/10.1016/j.jagp.2017.01.048
X
Referencias
Díaz-Gutiérrez MJ, Martínez-Cengotitabengoa M, Sáez de Adana E, Cano AI, Martínez- Cengotitabengoa MT, Besga A, et al. Relationship between the use of benzodiazepines and falls in older adults: A systematic review. Maturitas. 2017;101:17–22. https://doi.org/10.1016/j.maturitas.2017.04.002
X
Referencias
Ríos-Fraustro C, Galván-Plata ME, Gómez-Galicia DL, Giraldo-Rodríguez L, Agudelo-Botero M, Mino-León D. Intrinsic and extrinsic factors associated with falls in older adults: a case-control study in Mexico. Gac Med Mex. 2020;157:127-132. https://doi.org/10.24875/gmm.m21000537
X
Referencias
Maroto-Rodriguez J, Delgado-Velandia M, Ortolá R, García-Esquinas E, Martinez-Gomez D, Struijk EA, et al. A Mediterranean Lifestyle and Frailty Incidence in Older Adults: The Seniors- ENRICA-1 Cohort. The Journal of Gerontology. 2022;77(9):1845–52. https://doi.org/10.1093/gerona/glab292
X
Referencias
Concha-Cisternas Y, Vargas-Vitoria R, Celis-Morales C. Morphophysiological changes and fall risk in the older adult: A review of the literature. Revista Salud Uninorte. 2020;36(2):450–70. https://doi.org/10.14482/sun.36.2.618.97
-
World Health Organization. A Global Report on Falls Prevention Epidemiology of Falls A Global Report on Falls Prevention Epidemiology of Falls Sachiyo Yoshida-Intern Ageing and Life Course Family and Community Health World Health Organization. [Internet] [Cited: 2008 March 17] Available from: https://extranet.who.int/agefriendlyworld/wp-content/uploads/2014/06/WHo-Global-report-on-falls-prevention-in-older-age.pdf
-
Pfortmueller CA, Lindner G, Exadaktylos AK. Reducing fall risk in the elderly: risk factors and fall prevention, a systematic review. Minerva Med. 2014;105(4):275-81. https://pubmed.ncbi.nlm.nih.gov/24867188/
-
Burns ER, Stevens JA, Lee R. The direct costs of fatal and non-fatal falls among older adults — United States. J Safety Res. 2016;58:99–103. https://doi.org/10.1016/j.jsr.2016.05.001
-
Pinheiro A, Schmidt AM, Simon C, Moura CMAB, Guerra D, Klipel GDS, et al. Economic overview of falls among elderly Brazilians. Epidemiologia e Servicos de Saude. Ministry of Health; 2022;31(2):e2022536. https://doi.org/10.1590/S2237-96222022000200024
-
Bunt CW, Hogan AJ. The Effect of Statins on Dementia and Cognitive Decline. American Family Physician. 2017;95(3):151-152. https://www.aafp.org/pubs/afp/issues/2017/0201/p151.html
-
Lavedán Santamaría A, Jürschik Giménez P, Botigué Satorra T, Nuin Orrio C, Viladrosa Montoy M. Prevalencia y factores asociados a caídas en adultos mayores que viven en la comunidad. Aten Primaria. 2015;47(6):367–375. https://doi.org/10.1016/j.aprim.2014.07.012
-
Organización Mundial de la Salud. Subsanar las desigualdades en una generación: Alcanzar la equidad sanitaria actuando sobre los determinantes sociales de la salud: resumen analítico del informe final. Consulta: Agosto 27, 2008. Disponible en: https://www.who.int/es/publications/i/item/WHO-IER-CSDH-08.1
-
Garin N, Olaya B, Perales J, Moneta MV, Miret M, Ayuso-Mateos JL, et al. Multimorbidity patterns in a national representative sample of the Spanish adult population. PLoS One. 2014;9(1):e0123037. https://doi.org/10.1371/journal.pone.0084794
-
Ang GC, Low SL, How CH. Approach to falls among the elderly in the community. Singapore Med J. 2020;61(3):116–121. https://doi.org/10.11622/smedj.2020029
-
Clegg A, Young J, Iliffe S, Rikkert MO, Rockwood K. Frailty in elderly people. In: The Lancet. 2013;381(9868):752–762. http://dx.doi.org/10.1016/S0140-6736(12)62167-9
-
Milos V, Bondesson Å, Magnusson M, Jakobsson U, Westerlund T, Midlöv P. Fall risk-increasing drugs and falls: a cross-sectional study among elderly patients in primary care. BMC Geriatric. 2014;40:14. https://doi.org/10.1186/1471-2318-14-40
-
Herr M, Robine JM, Aegerter P, Arvieu JJ, Ankri J. Contribution of socioeconomic position over life to frailty differences in old age: comparison of life-course models in a French sample of 2350 old people. Ann Epidemiol. 2015;25(9):674-680. https://doi.org/10.1016/j.annepidem.2015.05.006
-
Petronila Gómez L, Aragón Chicharro S, Calvo Morcuende B. Caídas en ancianos institucionalizados: valoración del riesgo, factores relacionados y descripción. Gerokomos. 1990;28(1):2–8. Available from: https://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S1134-928X2017000100002&lng=es&nrm=iso&tlng=pt
-
Otani H, Shimoinaba J, Kashiwagi H, Morita T, Maeda I, Yokomichi N, et al. Prevalence of falls in the last weeks of life and relationship between falls, independence and quality of dying in Japan: a large prospective cohort study. BMJ Open. 2024;14:e085315. https://doi.org/10.1136/bmjopen-2024-085315
-
De Vries OJ, Peeters GMEE, Lips P, Deeg DJH. Does frailty predict increased risk of falls and fractures? A prospective population-based study. Osteoporos Int. 2013;24:2397-2403. https://doi.org/10.1007/s00198-013-2303-z
-
Nakanishi N, Nakura I, Nagano K, Yoneda H, Takatorige T, Shinsho F, et al. Mortality in Relation to The Type of Household Among Elderly People Living in a Community. Journal of Epidemiology. 1998;8(1):65-72. https://doi.org/10.2188/jea.8.65
-
Davis JC, Husdal K, Rice J, Loomba S, Falck RS, Dimri V, et al. Cost-effectiveness of falls prevention strategies for older adults: protocol for a living systematic review. BMJ Open. 2024;14(11):e088536. http://www.ncbi.nlm.nih.gov/pubmed/39500610. https://doi.org/10.1136/bmjopen-2024-088536
-
Guallar-Castillón P, Gil-Montero M, León-Muñoz LM, Graciani A, Bayán-Bravo A, Taboada JM, et al. Magnitude and management of hypercholesterolemia in the adult population of Spain, 2008- 2010: The ENRICA study. Rev Esp Cardiol. 2012;65(6):551–8. https://doi.org/10.1016/j.rec.2012.03.001
-
Rodríguez-Artalejo F, Graciani A, Guallar-Castillón P, León-Muñoz LM, Zuluaga MC, López-García E, et al. Justificación y métodos del estudio sobre nutrición y riesgo cardiovascular en España (ENRICA). Rev Esp Cardiol. 2011;64(10):876–82. https://doi.org/10.1016/j.recesp.2011.05.019
-
Zuluaga MC, Guallar-Castillón P, Conthe P, Rodríguez-Pascual C, Graciani A, León-Muñoz LM, et al. Housing conditions and mortality in older patients hospitalized for heart failure. American Heart Journal. 2011;161(5):950–5. https://doi.org/10.1016/j.ahj.2011.03.002
-
Alter DA, Yu W. The Burgeoning Roots of Socioeconomic Inequalities in Health: The Legacy Effect. Revista Española de Cardiología. 2017;70(3):138–139. https://doi.org/10.1016/j.rec.2016.08.006
-
McMunn A, Nazroo J, Breeze E. Inequalities in health at older ages: a longitudinal investigation of the onset of illness and survival effects in England. Age and Ageing. 2009;38(2):181-187.https://doi.org/10.1093/ageing/afn236
-
Aromaa A, Koponen P, Tafforeau J, Vermeire C. Evaluation of Health Interview Surveys and Health Examination Surveys in the European Union. European Journal of Public Health. 2003;13(1):67-72. https://doi.org/10.1093/eurpub/13.suppl_1.67
-
Instituto Nacional de Estadística. Clasificación nacional de ocupaciones 2011. Consulta: Noviembre 11, 2010.
-
Salcedo Salgado JD. Data Base Enrica Senior I. Mendeley V1. 2025.
-
Khow KSF, Visvanathan R. Falls in the Aging Population. Clin Geriatr Med. 2017;33(3):357-368. https://doi.org/10.1016/j.cger.2017.03.002
-
Enderlin C, Rooker J, Ball S, Hippensteel D, Alderman J, Fisher SJ, et al. Summary of factors contributing to falls in older adults and nursing implications. Geriatr Nurs. 2015 ;36(5):397–406. https://doi.org/10.1016/j.gerinurse.2015.08.006
-
Lander E. Crisis civilizatoria, límites del planeta, asaltos a la democracia y pueblos en resistencia. 2015. Consulta: Septiembre 5, 2015. Disponible en: https://doi.org/10.22201/cela.24484946e.2015.36.52598
-
Morrison S, Colberg SR, Parson HK, Neumann S, Handel R, Vinik EJ, et al. Walking-Induced Fatigue Leads to Increased Falls Risk in Older Adults. J Am Med Dir Assoc. 2016;17(5):402–409. https://doi.org/10.1016/j.jamda.2015.12.013
-
Mata García C, López-Espinosa Plaza A. Estudio del riesgo de caídas en pacientes orto- geriátricos. Revista Enfermería Docente 2017;(108):12-15. https://dialnet.unirioja.es/servlet/articulo?codigo=10624489
-
Martinez-Cengotitabengoa M, Diaz-Gutierrez MJ, Besga A, Bermúdez-Ampudia C, López P, Rondon MB, et al. Benzodiazepine prescriptions and falls in older men and women. Revista de Psiquiatría y Salud Mental. 2018;11(1):12–8. https://doi.org/10.1016/j.rpsm.2017.01.004
-
Seitz D, Iaboni A, Kirkham J. Psychotropic Drugs and Falls in Older Adults: an Update for the Geriatric Psychiatrist. The American Journal of Geriatric Psychiatry. 2017;25(3). https://doi.org/10.1016/j.jagp.2017.01.048
-
Díaz-Gutiérrez MJ, Martínez-Cengotitabengoa M, Sáez de Adana E, Cano AI, Martínez- Cengotitabengoa MT, Besga A, et al. Relationship between the use of benzodiazepines and falls in older adults: A systematic review. Maturitas. 2017;101:17–22. https://doi.org/10.1016/j.maturitas.2017.04.002
-
Olivares B, Rossi Munilla A, Herrmann-Lunecke MG. The walks of the elderly through their neighborhoods of residence in Santiago, Chile. Psicoperspectivas. 2022;21(3). https://doi.org/10.5027/psicoperspectivas-Vol21-Issue3-fulltext-2754
-
Ríos-Fraustro C, Galván-Plata ME, Gómez-Galicia DL, Giraldo-Rodríguez L, Agudelo-Botero M, Mino-León D. Intrinsic and extrinsic factors associated with falls in older adults: a case-control study in Mexico. Gac Med Mex. 2020;157:127-132. https://doi.org/10.24875/gmm.m21000537
-
Maroto-Rodriguez J, Delgado-Velandia M, Ortolá R, García-Esquinas E, Martinez-Gomez D, Struijk EA, et al. A Mediterranean Lifestyle and Frailty Incidence in Older Adults: The Seniors- ENRICA-1 Cohort. The Journal of Gerontology. 2022;77(9):1845–52. https://doi.org/10.1093/gerona/glab292
-
Concha-Cisternas Y, Vargas-Vitoria R, Celis-Morales C. Morphophysiological changes and fall risk in the older adult: A review of the literature. Revista Salud Uninorte. 2020;36(2):450–70. https://doi.org/10.14482/sun.36.2.618.97