Rev Cuid. 2026; 17(1): 5426
Abstract
Introduction: Endometriosis is a chronic inflammatory disease that affects 10% of women, causing pelvic pain, dysmenorrhea, and infertility, with a strong impact on quality of life. Objective: To analyze the current scientific evidence on the influence of diet and physical exercise on symptoms and quality of life in women of reproductive age with endometriosis. Materials and Methods: A systematic review of studies published between 2014 and 2024 was conducted using the descriptors endometriosis, exercise, diet, and quality of life in the following databases: MEDLINE, Web of Science, Scopus, SciELO, Virtual Health Library, Dialnet, and Cochrane Library. Systematic reviews, meta-analyses, case reports, letters, and articles without full-text access were excluded. Two independent reviewers performed study selection and data extraction, and methodological quality was assessed according to study design. Results: Of 523 initial records, 13 articles were included (7 on diet and 6 on exercise). Anti-inflammatory dietary interventions and regular physical exercise were associated with reduced symptoms and improved quality of life. Discussion: Diet and exercise may influence the symptoms and well-being of these patients, although the evidence is limited and inconsistent. The included studies show methodological heterogeneity, small sample sizes, and variability in interventions and outcomes, limiting internal validity and the generalizability of the findings. Conclusions: Diet and exercise constitute complementary strategies to pharmacological and/or surgical treatment within a comprehensive approach to endometriosis; however, more rigorous research is needed to support their long-term benefits.
Keywords: Endometriosis; Exercise; Diet; Quality of Life; Systematic Review.
Resumen
Introducción: La endometriosis es una enfermedad inflamatoria crónica que afecta al 10% de las mujeres, provocando dolor pélvico, dismenorrea e infertilidad, con un impacto significativo en la calidad de vida. Objetivo: Analizar la evidencia científica actual sobre la influencia de la dieta y ejercicio físico, en los síntomas y la calidad de vida de mujeres en edad fértil con endometriosis. Materiales y Métodos: Se realizó una revisión sistemática de estudios publicados entre 2014 y 2024, usando los descriptores endometriosis, exercise, diet y quality of life, en las siguientes bases de datos: Medline, Web of Science, Scopus, Scielo, Biblioteca Virtual de Salud, Dialnet y Cochrane. Se excluyeron revisiones sistemáticas, metaanálisis, casos clínicos, cartas y artículos sin acceso completo. Dos revisores independientes realizaron selección y extracción de datos, evaluando la calidad metodológica según el tipo de estudio. Resultados: De 523 registros iniciales, se seleccionaron 13 artículos (7 sobre dieta y 6 sobre ejercicio). Intervenciones dietéticas antiinflamatorias y ejercicio físico regular se asociaron con reducción de síntomas y mejoría en la calidad de vida. Discusión: Dieta y ejercicio pueden influir en los síntomas y bienestar de estas pacientes, aunque la evidencia es limitada e inconsistente. Los estudios presentan heterogeneidad metodológica, muestras pequeñas y variabilidad en las intervenciones y resultados, limitando la validez interna y la generalización de los hallazgos. Conclusiones: Dieta y ejercicio constituyen estrategias complementarias al tratamiento farmacológico y/o quirúrgico dentro de un abordaje integral de la endometriosis, si bien se precisa investigación más rigurosa que respalde sus beneficios a largo plazo.
Palabras Clave: Endometriosis; Ejercicio Físico; Dieta; Calidad de Vida; Revisión Sistemática.
Resumo
Introdução: A endometriose é uma doença inflamatória crónica que afeta 10% das mulheres, provocando dor pélvica, dismenorreia e infertilidade, com forte impacto na qualidade de vida. Objetivo: Avaliar as evidências científicas atuais sobre a influência da dieta e do exercício físico nos sintomas e na qualidade de vida de mulheres em idade fértil com endometriose. Materiais e Métodos: Foi realizada uma revisão sistemática de estudos publicados entre 2014 e 2024, utilizando os descritores endometriose, exercício físico, dieta e qualidade de vida, nas seguintes bases de dados: Medline, Web of Science, Scopus, SciELO, Biblioteca Virtual em Saúde, Dialnet e Cochrane. Revisões sistemáticas, meta-análises, relatos de caso, cartas e artigos sem acesso completo foram excluídos. Dois revisores independentes realizaram a seleção e extração de dados, avaliando a qualidade metodológica de acordo com o tipo de estudo. Resultados: De 523 registros iniciais, 13 artigos foram selecionados (7 sobre dieta e 6 sobre exercício físico). Intervenções dietéticas anti-inflamatórias e exercícios físicos regulares foram associados à redução dos sintomas e à melhora da qualidade de vida. Discussão: Dieta e exercícios podem influenciar os sintomas e o bem-estar dessas pacientes, embora as evidências sejam limitadas e inconsistentes. Os estudos apresentam heterogeneidade metodológica, amostras pequenas e variabilidade nas intervenções e nos desfechos, o que limita a validade interna e a generalização dos resultados. Conclusões: Dieta e exercícios são estratégias complementares ao tratamento farmacológico e/ou cirúrgico dentro de uma abordagem abrangente para a endometriose, embora sejam necessárias pesquisas mais rigorosas para comprovar seus benefícios a longo prazo.
Palavras-Chave: Endometriose; Exercício Físico; Dieta; Qualidade de Vida; Revisão Sistemática.
Introduction
Endometriosis is a chronic, estrogen-dependent inflammatory disease characterized by the presence of endometrial-like tissue outside the uterine cavity. Its etiology is multifactorial, involving genetic, immunological, and environmental factors1-3. It affects approximately 10% of women of reproductive age worldwide4,5, with a significant impact on physical and emotional health and quality of life4. Its prevalence varies across regions due to differences in health systems, cultural factors, and socioeconomic conditions. In Colombia, population-based studies are lacking; however, patient associations report that approximately 3.5 million women are affected6.
Clinically, chronic pelvic pain, severe dysmenorrhea, and dyspareunia predominate, occurring in up to 75% of cases. Menstrual disorders and infertility are also common, with infertility affecting up to 40% of diagnosed women1,2,4,7. On physical examination, findings may include a retroverted (tilted) uterus, pelvic tenderness, and enlarged ovaries6. Pain and infertility are key symptoms guiding the diagnostic assessment2,7.
Endometriosis is classified according to lesion location and depth of infiltration: superficial (type I), characterized by small lesions; ovarian (type II), characterized by endometriomas; and deep infiltrating endometriosis (type III), characterized by nodules >5 mm5,7. Diagnosis is based on medical history, physical examination, and imaging modalities (such as ultrasound or magnetic resonance imaging), although definitive diagnosis remains laparoscopic7. Factors such as family history, early menarche, and short menstrual cycles are associated with increased risk7.
Endometriosis management requires a multidisciplinary approach aimed at relieving pain, preserving fertility, and improving quality of life. There is no curative treatment; management focuses on slowing disease progression and controlling symptoms through pharmacological, surgical, or combined approaches4,7,8. Hormonal therapies (combined oral contraceptives, progestins, and gonadotropin- releasing hormone [GnRH] analogs) temporarily reduce estrogenic stimulation of ectopic tissue, and surgery is indicated only in refractory cases or when malignancy is suspected7.
Proinflammatory diets, physical inactivity, and low antioxidant intake have been associated with more severe disease2,8-10. Diet may modulate estrogen levels, promote a healthy gut microbiota, and reduce proinflammatory prostaglandins and cytokines11-13. Likewise, antioxidant supplementation may reduce symptoms10.
Physical exercise is defined as planned and repetitive bodily activity performed to improve physical fitness14. In animal models, reductions in proinflammatory myokines have been observed following training15. Regular exercise may decrease cytokines such as TNF-α and IL-6, as well as circulating estrogen levels, thereby reducing stimulation of ectopic tissue and attenuating inflammation16,17. Pelvic floor muscle training has traditionally been recommended for women with chronic pelvic pain5, and recent studies suggest modulatory effects on pain and inflammation14,15.
Dietary habits and physical activity may have a positive effect on symptom control and quality of life in women with endometriosis by modulating inflammatory, hormonal, and immunological processes associated with the disease. This review aims to analyze how lifestyle modifications, particularly in diet and physical exercise, may contribute to symptom control and improved quality of life in women with endometriosis.
Materials and Methods
A systematic review was conducted in accordance with the PRISMA 2020 statement (Preferred Reporting Items for Systematic Reviews and Meta-Analyses). This review was not registered. As this study is a systematic review of previously published research, ethics committee approval was not required. No individual patient data or confidential information was used.
The research question was formulated according to the PICO framework Table 1 and aims to assess whether, among women of reproductive age diagnosed with endometriosis, dietary patterns and physical exercise are associated with differences in symptoms and quality of life, beyond standard symptomatic treatment.
Original studies published in English, Spanish, French and Portuguese between 2014 and 2024 that addressed diet or physical exercise in patients with a diagnosis of endometriosis were included. Reviews, case reports, or case series, letters to the editor, conference abstracts, and articles without full-text access were excluded.
Table 1. PICO Framework
X
Table 1. PICO Framework
| P (population) |
Women of reproductive age with a confirmed diagnosis of endometriosis |
| I (intervention) |
Patients’ dietary habits and food patterns Patients’ physical activity |
| C (comparison) |
Conventional pharmacological and/or surgical treatment of the disease |
| O (Outcomes) |
Patients’ symptoms Women’s quality of life |
The literature search was conducted in MEDLINE, Web of Science (WOS), Scopus, SciELO, Virtual Health Library, Dialnet, and the Cochrane Library. The search strategy included MeSH terms (“endometriosis,” “exercise,” “diet,” and “quality of life”) and DeCS descriptors (“endometriosis,” “diet,” “physical activity,” and “quality of life”), combined using Boolean operators (AND and OR) Table 2. The last search was performed on December 18, 2024.
Table 2. Search Strategy Across Databases
X
Table 2. Search Strategy Across Databases
| MEDLINE |
(("Endometriosis"[Mesh]) AND ("Exercise"[Mesh] OR "Diet"[Mesh])) (("Endometriosis"[Mesh]) AND ("Exercise"[Mesh] OR "Diet"[Mesh]) AND ("Quality of Life"[Mesh])) Filters: Clinical Study, Clinical Trial, Multicenter Study, Observational Study; Publication dates: 2014/01/01–2024/12/31 |
| Web of Science |
TS=("Endometriosis") AND TS=("Exercise" OR "Diet") AND TS=("Quality of Life") Refined by: Document Types = (ARTICLE OR CLINICAL TRIAL) Timespan: 2014–2024 |
| SciELO |
(“Endometriosis”) AND (“dieta” OR “ejercicio físico” OR “deporte”) (“Endometriosis”) AND (“dieta” OR “ejercicio físico” OR “deporte”) AND (“calidad de vida”) Filtered by: Articles; Publication years:2014–2024 |
| Scopus |
(TITLE-ABS-KEY("Endometriosis") AND TITLE-ABS-KEY("Exercise" OR "Diet") (TITLE-ABS-KEY("Endometriosis") AND TITLE-ABS-KEY("Exercise" OR "Diet") siAND TITLE-ABS-KEY("Quality of Life")) Filtered by: Article; Publication years 2014–2024 |
| Cochrane Library |
("Endometriosis" in Title Abstract Keyword) AND ("Exercise" OR "Diet" in Title Abstract Keyword) Filtered by: Trials; Publication years 2014–2024 |
| Virtual Health Library and Dialnet |
(Endometriosis) AND (“Ejercicio físico” OR “Dieta” OR "Calidad de vida") Filters: Publication years: 2014–2024 |
Two independent reviewers selected the studies in two stages: title and abstract screening, followed by full-text review of potentially eligible articles. Discrepancies were resolved by consensus. Zotero was used for reference management and duplicate removal, and the Rayyan platform facilitated study selection between reviewers. A standardized data extraction form was subsequently developed to collect relevant information from each study, including authors, year of publication, study design, sample characteristics, objectives, intervention and comparison group, and main outcomes.
Methodological quality and risk of bias were assessed using the Effective Public Health Practice Project Quality Assessment Tool (EPHPP) for quantitative studies and the Consolidated Criteria for Reporting Qualitative Research (COREQ) for qualitative research. According to the EPHPP, studies were classified as having strong, moderate, or weak methodological quality, while for the COREQ checklist, studies with < 50% item adherence were considered low quality and those with ≥75% adherence were considered high quality18,19. Discrepancies were resolved by consensus.
A descriptive analysis of the extracted data was conducted. The results are presented narratively and in tables, including relevant information from each study. All collected data are publicly available in Mendeley Data20.
Results
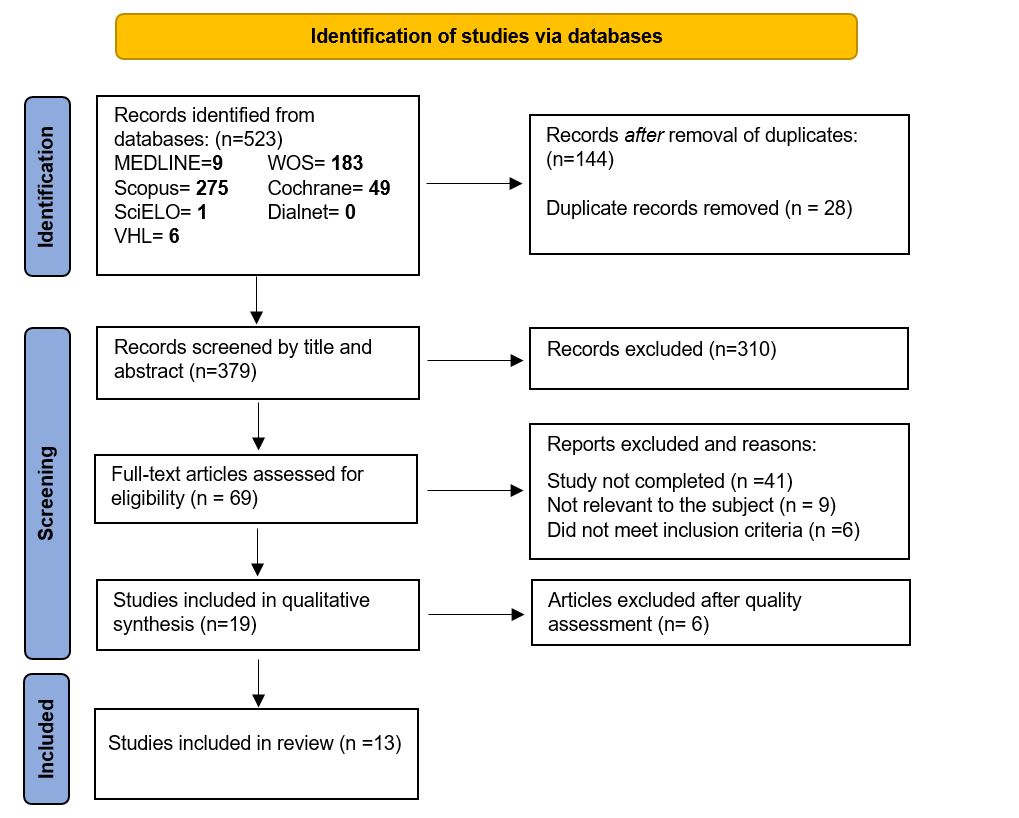
The initial search yielded a total of 523 records from databases including MEDLINE, Web of Science, Scopus, SciELO, the Virtual Health Library, and the Cochrane Library. After removal of duplicates (n = 144), an additional 310 records were excluded following title and abstract screening. A total of 69 articles were selected for full-text assessment Figure 1. This systematic review ultimately included 13 studies published between 2021 and 2024, encompassing various study designs: randomized controlled trials (n = 3), one quasi-experimental study (n = 1), observational studies (n = 8), and one qualitative study. Six studies focused on physical exercise-related outcomes, while seven addressed dietary habits or interventions. The main characteristics of these studies are presented in Table 3.
Several studies reported a positive association between dietary modification and improvement in symptom control or quality of life in women with endometriosis. Van Haaps et al.21 demonstrated, in a nonrandomized experimental study, that adherence to an endometriosis-specific diet or a low- FODMAP diet (low in fermentable oligosaccharides, disaccharides, monosaccharides, and polyols) over six months significantly reduced symptoms such as deep dyspareunia, dysuria, bloating, and fatigue. Improvements were also observed across multiple quality-of-life domains, including pain, functional limitation, emotional well-being, self-image, work life, and sexual relationships. Additionally, significant improvement in gastrointestinal health was observed, as assessed using the Gastrointestinal Quality of Life Index (GIQLI)22, whereas the control group showed no relevant changes.
Similarly, Ghasemisedaghat et al.2, in a case-control study, reported that higher adherence to the so-called “fertility diet,” characterized by high intake of plant protein, monounsaturated fats, and multivitamins, and low intake of animal protein, heme iron, and glycemic load, was associated with a significantly lower likelihood of endometriosis, suggesting a protective effect of certain dietary patterns. The likelihood of endometriosis was 82% and 69% lower in adjusted models with higher intake of plant protein and multivitamins, respectively. In contrast, high intake of animal protein, heme iron, and higher glycemic load were positively associated with an increased likelihood of endometriosis.
Other observational studies, such as van Haaps et al.4, showed that women who adhered to an “endometriosis diet,” characterized by the elimination of red meat, gluten, lactose, sugars, and estrogen-rich foods, had significantly higher scores across all quality-of-life domains (physical functioning, psychological functioning, spiritual well-being, overall quality of life, social participation, and daily functioning) compared with non-adherent women, particularly those with strict adherence. The main barriers to implementation included limited awareness and the complexity of the dietary intervention. Krabbenborg et al.8 reported that, although women with endometriosis had lower overall diet quality (as assessed using the DHD-15 index23) compared with a healthy population, those who implemented specific dietary modifications perceived a notable improvement in pain-related symptoms, particularly after eliminating gluten, dairy, or soy, or increasing vegetable intake.
From an inflammatory perspective, Liu et al.9, in a cross-sectional study of a large population-based sample, found that a higher dietary inflammatory index (DII) was associated with an increased risk of endometriosis. Women with endometriosis tended to have more proinflammatory diets, and those in the highest DII tertile had a 57% higher risk compared with those in the lowest DII tertile. These findings underscore the potential role of an anti-inflammatory diet in disease prevention.
Xie et al.3 also found that adequate serum vitamin D levels were inversely associated with the prevalence of endometriosis, even after adjustment for multiple confounders, supporting the immunomodulatory and anti-inflammatory role of this micronutrient.
In contrast, Li et al.10, using Mendelian randomization, found no evidence of a causal relationship between genetically determined circulating antioxidant levels and the risk of endometriosis. This suggests that antioxidant supplementation may not be effective as a preventive strategy in healthy populations, although its potential therapeutic role in affected patients cannot be ruled out.
Regarding physical exercise, several studies highlight its potential beneficial effects on pain symptoms and quality of life. Artacho-Cordón et al.24 evaluated a multimodal therapeutic exercise program in women with endometriosis refractory to conventional treatments, reporting significant improvements in quality of life, reduced dyspareunia, decreased pain catastrophizing and increased pain thresholds in the lumbopelvic region. With respect to pelvic floor physical therapy, Del Forno et al.5,25 published two studies based on a randomized controlled trial. A significant reduction in superficial dyspareunia and chronic pelvic pain was observed following the intervention. However, no significant differences were found in urinary, bowel, or sexual functioning, although a trend toward improvement in constipation was noted.
Ensari et al.1 observed that women who engaged in regular physical exercise (at least three times per week) were more likely to experience a reduction in pain following exercise, suggesting an analgesic effect associated with habitual physical activity. In contrast, Sachs et al.15 compared physical activity levels between women with and without endometriosis and found that those affected engaged in less exercise and lower levels of daily physical activity, even after adjusting for variables such as dysmenorrhea, depression, and use of hormonal contraceptives, which may reflect barriers related to pain or fatigue.
Finally, Tennfjord et al.14, in a qualitative study, reported that participants in a supervised exercise program, including strength training and pelvic floor muscle training, perceived exercise as a safe and empowering tool for self-management of the disease and for enhancing social support.
Table 3. Studies included in the systematic review
X
Table 3. Studies included in the systematic review
| Study |
Country |
Subject |
Study design |
Methodological quality and risk of bias |
Sample size |
Objectives |
Intervention |
Comparison |
Results |
| Xie et al. 20243 |
USA |
Diet |
Cross-sectional observational |
Weak |
3232 |
To examine the association between serum vitamin D levels and the presence of endometriosis |
None |
Comparison between women with adequate vs insufficient 25-hydroxyvitamin D3 levels |
A significant inverse association was found between adequate vitamin D levels and risk of endometriosis (OR 0.73; 95% CI 0.54–0.97). No significant differences were observed in carbohydrate intake or vitamin C intake between groups. |
| Li et al. 202410 |
China |
Diet |
Cross-sectional observational |
Moderate |
77,257 |
To assess the association between genetically determined circulating antioxidant levels and endometriosis risk |
None |
None |
Absolute circulating antioxidant levels (retinol, β-carotene, lycopene, vitamin C) were not significantly associated with endometriosis risk (OR 0.62–1.01). Circulating antioxidant metabolites (γ-tocopherol, α-tocopherol, retinol, vitamin C) also showed no significant associations per unit increase (OR 0.91–1.04) |
| van Haaps et al. 20234 |
Netherlands |
Diet |
Cross-sectional observational |
Weak |
211 |
To assess whether adherence to an endometriosis diet improves quality of life (“My Positive Health” questionnaire) in women with endometriosis |
None |
Comparison by level of adherence (strict, moderate, none) |
Women adhering to the diet reported better quality of life than non-adherent women, with significant differences in total quality-of-life scores (1.9 vs 2.3), symptoms (2.1 vs 2.5), and social functioning (1.8 vs 2.2). Women who followed the diet also experienced fewer gastrointestinal (2.0 vs 2.4) and menstrual symptoms (2.2 vs 2.6), with all comparisons showing statistically significant differences (p < 0.05). |
| Ghasemisedaghat et al. 20232 |
Iran |
Diet |
Case-control |
Moderate |
317 |
To examine the effects of a fertility diet on endometriosis. |
None |
107 cases with endometriosis vs 210 controls matched by age and other factors |
Women with higher fertility diet scores had lower odds of developing endometriosis (OR 0.44, 95% CI: 0.27–0.71, p = 0.001 in the crude model; OR 0.46, 95% CI: 0.23–0.90, p = 0.022 in the adjusted model). Favorable associations were identified between the fertility diet and intake of plant protein and multivitamins, as well as unfavorable associations with intake of animal protein, heme iron, and glycemic load. |
| Liu et al. 20239 |
USA. |
Diet |
Cross-sectional observational |
Weak |
3,410 |
To examine the association between dietary inflammatory index (DII) and endometriosis risk |
None |
Comparison between high vs low Dietary Inflammatory Index (DII) |
Higher inflammatory index was associated with a 57% higher prevalence of endometriosis, particularly among non-obese, non-diabetic, hypertensive women, oral contraceptive users, and non-nulliparous women. In adjusted models, the ORs for women in the DII third quartile compared with those in the DII first quartile ranged from 1.55 to 2.25, depending on subgroup characteristics. |
| Krabbenborg et al. 20218 |
Netherlands |
Diet |
Cross-sectional observational |
Weak |
157 |
To identify the dietary patterns followed by women with endometriosis and determine whether they perceive any effects on their disease. |
None |
None |
Women with endometriosis reported symptom improvement following dietary modifications implemented after diagnosis. The proportion of participants reporting symptom improvement after eliminating specific foods was as follows: gluten (75%), dairy (70%), and soy (65%). Additionally, 80% of participants reported symptom improvement after increasing vegetable intake, and 60% reported improvement after increasing fish consumption. |
| Tennfjord et al. 202414 |
Norway |
Physical exercise |
Qualitative |
Moderate |
41 |
To explore how physical activity and pelvic floor muscle training benefit women with endometriosis. |
A four-month program of supervised weekly group training and home-based individual sessions (3-5 sessions per week). |
Qualitative comparison pre-post intervention |
Training women in physical activity and pelvic floor muscle exercise contributed to an improved perceived quality of life. The individualized and supervised nature of the program was positively valued, with participants reporting reduced fear of exercise. |
| Sachs et al. 202315 |
Switzerland, Austria, Germany |
Physical exercise |
Cross-sectional observational |
Moderate |
920 |
To assess physical activity levels in women with and without endometriosis |
None |
Compares a group of women with surgically confirmed endometriosis with an age-matched group without suspected diagnosis. |
Women with endometriosis engaged in fewer weekly hours of moderate (48.5% vs 52.1%) and vigorous physical activity (22.3% vs 25.4%), even after adjustment for confounding variables. The proportion of sedentary women was higher in the endometriosis group (29.2% vs 22.5%). Endometriosis, dysmenorrhea, and depression were associated with lower levels of physical activity. |
| van Haaps et al. 202321 |
Netherlands |
Physical exercise |
Quasi-experimental |
Weak |
62 |
To evaluate whether the dietary intervention reduces pain and improves quality of life over six months |
Low-FODMAP diet or endometriosis-specific diet. |
Compares intervention group with control group and baseline values. |
A significant reduction in pain was observed in the intervention group, with no changes in the control group. Participants reported less deep dyspareunia (mean difference −1.15) and less abdominal bloating (mean difference −0.99) compared with the control group, with statistically significant differences. Women who followed the diet showed significant improvements in 6 of 11 EHP-30 domains (pain, control/powerlessness, emotional well-being, self-image, work, and sexual functioning), with no changes observed in the control group. |
| Artacho-Cordón et al. 202324 |
Spain |
Physical exercise |
Randomized controlled trial |
Moderate |
31 |
To evaluate the effectiveness of a supervised therapeutic exercise program in reducing pain, improving quality of life, and addressing lumbopelvic dysfunction in women with endometriosis. |
Eight-week supervised, progressive, and individually tailored exercise program. |
Standard medical treatment |
The program was highly satisfactory and well tolerated. Significant and sustained improvements at one year were observed in quality of life, pain, strength, stability, and muscle mass. Dyspareunia was reduced in 90% of women who adhered to the instructions. |
| Del Forno et al. 20235 |
Italy |
Physical exercise |
Randomized controlled trial |
Moderate |
30 |
To evaluate the effects of pelvic floor physiotherapy on urinary, bowel, and sexual function in deep infiltrating endometriosis |
Five individual sessions of pelvic floor physical therapy. |
No intervention; standard gynecological care. |
Regarding pain, no statistically significant differences were observed between the intervention and control groups compared with baseline (p = 0.665). No significant differences were found between the two groups in urinary, bowel, or sexual function; however, women in the intervention group showed a trend toward improvement in constipation symptoms. |
| Ensari et al. 20221 |
38 countries |
Physical exercise |
Cross-sectional observational |
Weak |
1009 |
To investigate the association of daily physical exercise with pain symptoms in endometriosis. |
None |
None |
A linear model was used to analyze the relationship between previous-day exercise and daily pain, with habitual exercise frequency functioning as moderator. Habitual exercise frequency showed a small but statistically significant moderating effect (rate ratio: 0.96 for total pain score; pain score difference coefficient: -0.14; p < 0.05). As habitual exercise frequency increased, the effect of previous-day exercise on daily pain became more favorable. Participants with lower frequency or no regular exercise reported higher pain levels and greater increases in pain intensity following exercise. |
| Del Forno et al. 202125 |
Italy |
Physical exercise |
Randomized controlled trial |
Moderate |
30 |
To evaluate pelvic floor muscle training on urinary, bowel, and sexual function in deep infiltrating endometriosis |
Five individual pelvic floor sessions |
No intervention; standard gynecological care. |
The intervention group showed a mean reduction of 3 points in superficial dyspareunia on the numeric rating scale (IQR −4, −2), with no change in the control group (p < 0.01). A statistically significant difference was also observed in the change in chronic pelvic pain, with median values of 0 (IQR −2, 0) in the intervention group and (IQR 0, 1) in the control group. |
Discussion
The results of this systematic review suggest that both physical exercise and dietary interventions may play a relevant role in reducing symptoms and improving quality of life in women with endometriosis. Several studies report significant benefits in terms of reductions in pelvic pain and dyspareunia, as well as improvements in physical and psychological well-being, particularly when structured therapeutic exercise programs or anti-inflammatory diets are implemented.
Regarding diet, the analyzed studies show heterogeneous approaches, with elimination of potentially proinflammatory foods, such as dairy products and red meat, being the most common approaches. These restrictions have demonstrated greater effectiveness in reducing symptoms, particularly pain, compared with the isolated use of supplements3,4,9. Dietary modifications appear to benefit primarily patients with established disease, without clear evidence of a significant preventive role, and show greater effectiveness when combined with conventional treatments10,26. Anti-inflammatory diets may improve symptom control by reducing inflammation, oxidative stress, and cellular proliferation27,28.
A major challenge is treatment adherence, which is often affected by the psychological burden of the disease and may reduce motivation to adopt new habits29. Additionally, there is still a lack of consensus regarding which foods should be eliminated, despite the increasing recommendation of endometriosis-specific diets4,30.
Regarding physical activity, women with endometriosis tend to engage in less exercise due to symptom-related interference with daily life, which limits their ability to engage in physical activity1,7,14,15,29. However, when exercise is incorporated, benefits in symptom reduction are observed, particularly among women who have undergone surgical treatment5. Up to 42% use physical activity as a self-management strategy, although many lack adequate training14.
The literature indicates that physical activity increases pain tolerance, modulates the inflammatory response, and provides psychological benefits, such as improved self-esteem and a greater sense of control over health, in addition to preventing comorbidities associated with physical inactivity1,14,15,31. Physical activity may act through multiple mechanisms, including activation of endogenous pain inhibition pathways, reduction of proinflammatory cytokines, improved sensitivity to estrogen and progesterone, reduction of stress and chronically elevated cortisol levels, as well as improved insulin sensitivity, increased sex hormone-binding globulin (SHBG), and reduced circulating estrogen levels16,17.
When considering lifestyle changes, the economic factor is relevant, as many women lack access to specialized healthcare professionals in the private sector. In this context, nurses can play a key role as educators and promoters of healthy behaviors by providing guidance on care and self-care, while nutritionists and physical therapists are essential for a comprehensive approach, although their availability within healthcare services remains limited4,30.
For healthcare professionals, the available evidence does not support making specific recommendations for or against non-medical interventions, including physical activity and dietary modifications, due to the low methodological quality of the studies, inconsistent results, and potentially undefined adverse effects32,33. Hormonal pharmacological treatment remains the cornerstone of endometriosis management, controlling endometrial tissue proliferation, alleviating pain, improving fertility, and reducing bleeding7. However, healthcare professionals should discuss with patients the possibility of incorporating non-pharmacological strategies as part of a comprehensive, person-centered approach, prioritizing shared decision-making, as these interventions may represent a beneficial option despite the existing uncertainty7,34-36. Exercise and physical activity may be considered components of a healthy lifestyle, although high-quality clinical trials demonstrating their specific effectiveness on disease symptoms are lacking37. Therefore, current clinical guidelines and professional societies do not recommend any specific non-medical intervention for endometriosis management, highlighting the need for further high-quality research in this field32,33,36,37.
This systematic review provides a comprehensive analysis of the recent literature on diet and exercise in women with endometriosis. Key strengths include a broad search strategy, inclusion of studies with diverse designs (randomized controlled trials, observational studies, and qualitative research), and systematic assessment of methodological quality and risk of bias using tools such as EPHPP and COREQ. This approach provides a comprehensive overview of the current state of the evidence, identifying consistent findings as well as areas of uncertainty.
When interpreting the results, several limitations should be considered. This systematic review included a relatively small number of studies, which may reflect the need for further research in this area. In addition, the protocol was not registered a priori, which may affect transparency. Methodological diversity among the included studies, heterogeneity in the interventions applied, and the use of different instruments to assess clinical outcomes hinder comparability across studies and reduce the external validity of the findings. Many studies included small sample sizes, nonrandomized designs, and a limited number of prospective studies, which increases the risk of bias and limits the ability to establish clear causal relationships. Publication bias cannot be ruled out, as studies with null or negative results may not have been published.
Future research should focus on multicenter randomized controlled trials with larger sample sizes and long-term follow-up, incorporating standardized measures of clinical outcomes and further elucidating the underlying pathophysiological mechanisms, thereby enabling the development of evidence-based recommendations.
Conclusions
Current evidence suggests that lifestyle factors, such as diet and physical activity, may influence symptoms and quality of life in women with endometriosis. Non-pharmacological interventions, including regular physical exercise and the adoption of anti-inflammatory diets, may help reduce symptom severity and improve quality-of-life markers. However, further high-quality research is needed to establish robust evidence for this therapeutic approach and its long-term benefits.
Conflict of Interest: The authors declare no conflicts of interest related to this article.
Funding: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
X
Referencias
Ensari I, Lipsky-Gorman S, Horan EN, Bakken S, Elhadad N. Associations between physical exercise patterns and pain symptoms in individuals with endometriosis: a cross-sectional mHealth-based investigation. BMJ Open. 2022;12(7):e059280. https://doi.org/10.1136/bmjopen-2021-059280
X
Referencias
Ghasemisedaghat S, Eslamian G, Kazemi SN, Rashidkhani B, Taheripanah R. Association of fertility diet score with endometriosis: a case–control study. Frontiers in Nutrition. 2023;10:1222018. https://doi.org/10.3389/fnut.2023.1222018
X
Referencias
Xie B, Liao M, Huang Y, Hang F, Ma N, Hu Q. Association between vitamin D and endometriosis among American women: National Health and Nutrition Examination Survey. PLoS ONE. 2024;19(1):e0296190. https://doi.org/10.1371/journal.pone.0296190
X
Referencias
van Haaps A, Wijbers J, Schreurs A, Mijatovic V. A better quality of life could be achieved by applying the endometriosis diet: a cross-sectional study in Dutch endometriosis patients. Reprod Biomed Online. 2023;46(3):623–630. https://doi.org/10.1016/j.rbmo.2022.12.010
X
Referencias
Del Forno S, Cocchi L, Arena A, Pellizzone V, Lenzi J, Raffone A, et al. Effects of Pelvic Floor Muscle Physiotherapy on Urinary, Bowel, and Sexual Functions in Women with Deep Infiltrating Endometriosis: A Randomized Controlled Trial. Medicina (Kaunas). 2023;60(1):67. https://doi.org/10.3390/medicina60010067
X
Referencias
Ministerio de Sanidad, Servicios Sociales e Igualdad. Guía de atención a las mujeres con endometriosis en el Sistema Nacional de Salud (SNS), 2013. Madrid (España). Consulta: Junio 26, 2025.
X
Referencias
Krabbenborg I, de Roos N, van der Grinten P, Nap A. Diet quality and perceived effects of dietary changes in Dutch endometriosis patients: an observational study. Reprod Biomed Online. 2021;43(5):952–61. https://doi.org/10.1016/j.rbmo.2021.07.011
X
Referencias
Liu P, Maharjan R, Wang Y, Zhang Y, Zhang Y, Xu C, et al. Association between dietary inflammatory index and risk of endometriosis: A population-based analysis. Frontiers in Nutrition. 2023;10:1077915. https://doi.org/10.3389/fnut.2023.1077915
X
Referencias
Li X, Xie Z, Qiu H, Xie X, Liu L. Exploring the causal associations between diet-derived circulating antioxidants and the risk of endometriosis: a Mendelian randomization study. Frontiers in Nutrition. 2024;11:1453147. https://doi.org/10.3389/fnut.2024.1453147
X
Referencias
Brouns F, Van Haaps A, Keszthelyi D, Venema K, Bongers M, Maas J, et al. Diet associations in endometriosis: a critical narrative assessment with special reference to gluten. Front Nutr. 2023;10:1295983. https://doi.org/10.3389/fnut.2023.1166929
X
Referencias
Qin R, Tian G, Liu J, Cao L. The gut microbiota and endometriosis: From pathogenesis to diagnosis and treatment. Front Cell Infect Microbiol. 2022;12:1069557. https://doi.org/10.3389/fcimb.2022.1069557
X
Referencias
Tennfjord MK, Gabrielsen R, Bø K, Engh ME, Molin M. Can general exercise training and pelvic floor muscle training be used as an empowering tool among women with endometriosis? Experiences among women with endometriosis participating in the intervention group of a randomized controlled trial. BMC Womens Health. 2024;24:505. https://doi.org/10.1186/s12905-024-03356-w
X
Referencias
Sachs MK, Dedes I, El-Hadad S, Haufe A, Rueff D, Kohl Schwartz AS, et al. Physical Activity in Women with Endometriosis: Less or More Compared with a Healthy Control?. Int J Environ Res Public Health. 2023;20(17):6659. https://doi.org/10.3390/ijerph20176659
X
Referencias
Tennfjord MK, Gabrielsen R, Tellum T. Effect of physical activity and exercise on endometriosis-associated symptoms: a systematic review. BMC Women's Health. 2021;21(1):355. https://doi.org/10.1186/s12905-021-01500-4
X
Referencias
Martire FG, Costantini E, d’Abate C, Capria G, Piccione E, Andreoli A. Endometriosis and Nutrition: Therapeutic Perspectives. J. Clin. Med. 2025;14(11):3987. . https://doi.org/10.3390/jcm14113987
X
Referencias
Thomas BH, Ciliska D, Dobbins M, Micucci S. A process for systematically reviewing the literature: providing the research evidence for public health nursing interventions. Worldviews Evid Based Nurs. 2004;1(3):176-84. https://doi.org/10.1111/j.1524-475X.2004.04006.x
X
Referencias
Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. International Journal for Quality in Health Care. 2007;19(6):349–57. https://doi.org/10.1093/intqhc/mzm042
X
Referencias
Fuentes Rodríguez A, Grela Beres O. Análisis de artículos del impacto de dieta y ejercicio físico en endometriosis. 2025. Mendeley Data: Versión 1. https://doi.org/10.17632/mky2ntyknm.1
X
Referencias
Van Haaps AP, Wijbers JV, Schreurs AMF, Vlek S, Tuynman J, Bie BD, et al. The effect of dietary interventions on pain and quality of life in women diagnosed with endometriosis: a prospective study with control group. Hum Reprod. 2023;38(12):2433-2446. https://doi.org/10.1093/humrep/dead214
X
Referencias
Eypasch E, Williams JI, Wood-Dauphinee S, Ure BM, Schmülling C, Neugebauer E, et al. Gastrointestinal Quality of Life Index: development, validation and application of a new instrument. British Journal Surgery 1995;82(2):216–22. https://doi.org/10.1002/bjs.1800820229
X
Referencias
Looman M, Feskens EJ, Rijk M de, Meijboom S, Biesbroek S, Temme EH, et al. Development and evaluation of the Dutch Healthy Diet index 2015. Public Health Nutrition. 2017; 20(13):2289–99. https://doi.org/10.1017/S136898001700091X
X
Referencias
Artacho-Cordón F, Salinas-Asensio MDM, Galiano-Castillo N, Ocón-Hernández O, Peinado FM, Mundo-López A, et al. Effect of a Multimodal Supervised Therapeutic Exercise Program on Quality of Life, Pain, and Lumbopelvic Impairments in Women With Endometriosis Unresponsive to Conventional Therapy: A Randomized Controlled Trial. Arch Phys Med Rehabil. 2023;104(11):1785–95. https://doi.org/10.1016/j.apmr.2023.06.020
X
Referencias
Del Forno S, Arena A, Pellizzone V, Lenzi J, Raimondo D, Cocchi L, et al. Assessment of levator hiatal area using 3D/4D transperineal ultrasound in women with deep infiltrating endometriosis and superficial dyspareunia treated with pelvic floor muscle physiotherapy: randomized controlled trial. Ultrasound Obstet Gynecol. 2021;57(5):726–32. https://doi.org/10.1002/uog.23590
X
Referencias
Nodler JL, Divasta AD, Vitonis AF, Karevicius S, Malsch M, Sarda V, et al. Supplementation with vitamin D or ω-3 fatty acids in adolescent girls and young women with endometriosis (SAGE): A double-blind, randomized, placebo-controlled trial. Am J Clin Nutr. 2020;112(1):229–36. https://doi.org/10.1093/ajcn/nqaa096
X
Referencias
Barrea L, Verde L, Annunziata G, Chedraui P, Petraglia F, Cucalón G, et al. Effectiveness of Medical Nutrition Therapy in the Management of Patients with Obesity and Endometriosis: from the Mediterranean Diet To the Ketogenic Diet, Through Supplementation. The Role of the Nutritionist in Clinical Management. Curr Obes Rep. 2025;14:68. https://doi.org/10.1007/s13679-025-00662-8
X
Referencias
Baradwan S, Gari A, Sabban H, Alshahrani MS, Khadawardi K, Bukhari IA, et al. The effect of antioxidant supplementation on dysmenorrhea and endometriosis-associated painful symptoms: a systematic review and meta-analysis of randomized clinical trials. Obstet Gynecol Sci. 2024;67(2):186-98. https://doi.org/10.5468/ogs.23210
X
Referencias
Nap A, de Roos N. Endometriosis and the effects of dietary interventions: what are we looking for?. Reproduction and Fertility. 2022;3(2):C14–22. https://doi.org/10.1530/RAF-21-0110
X
Referencias
Salinas-Asensio MdM, Ocón-Hernández O, Mundo-López A, Fernández-Lao C, Peinado FM, Padilla-Vinuesa C, et al. “Physio-EndEA” Study: A Randomized, Parallel-Group Controlled Trial to Evaluate the Effect of a Supervised and Adapted Therapeutic Exercise Program to Improve Quality of Life in Symptomatic Women Diagnosed with Endometriosis. Int J Environ Res Public Health. 2022;19(3):1738. https://doi.org/10.3390/ijerph19031738
X
Referencias
Leroy R, Desimpel F, Ombelet S, De Jaeger M, Benahmed N, Camberlin C, et al. How can we improve endometriosis care in Belgium? KCE Report 378. Brussels (BE): Belgian Health Care Knowledge Centre (KCE); 2024. Consulta: octubre 10, 2025.
X
Referencias
Carvalho N, Margatho D, Cursino K, Benetti-Pinto CL, Bahamondes L. Control of endometriosis-associated pain with etonogestrel-releasing contraceptive implant and 52-mg levonorgestrel-releasing intrauterine system: randomized clinical trial. Fertil Steril. 2018;110(6):1129–36. https://doi.org/10.1016/j.fertnstert.2018.07.003
X
Referencias
Harada T, Kobayashi T, Hirakawa A, Takayanagi T, Nogami M, Mochiyama T, et al. Efficacy and safety of the combination of estetrol 15 mg/drospirenone 3 mg in a cyclic regimen for the treatment of endometriosis-associated pain and objective gynecological findings: a multicenter, placebo-controlled, double-blind, randomized study. Fertil Steril. 2024;122(5):894–901. https://doi.org/10.1016/j.fertnstert.2024.07.011
X
Referencias
Lee HJ, Yoon SH, Lee JH, Chung YJ, Park SY, Kim SW, et al. Clinical evaluation and management of endometriosis: 2024 guideline for Korean patients from the Korean Society of Endometriosis. Obstet Gynecol Sci. 2024;68(1):43-58. https://doi.org/10.5468/ogs.24242
-
Ensari I, Lipsky-Gorman S, Horan EN, Bakken S, Elhadad N. Associations between physical exercise patterns and pain symptoms in individuals with endometriosis: a cross-sectional mHealth-based investigation. BMJ Open. 2022;12(7):e059280. https://doi.org/10.1136/bmjopen-2021-059280
-
Ghasemisedaghat S, Eslamian G, Kazemi SN, Rashidkhani B, Taheripanah R. Association of fertility diet score with endometriosis: a case–control study. Frontiers in Nutrition. 2023;10:1222018. https://doi.org/10.3389/fnut.2023.1222018
-
Xie B, Liao M, Huang Y, Hang F, Ma N, Hu Q. Association between vitamin D and endometriosis among American women: National Health and Nutrition Examination Survey. PLoS ONE. 2024;19(1):e0296190. https://doi.org/10.1371/journal.pone.0296190
-
van Haaps A, Wijbers J, Schreurs A, Mijatovic V. A better quality of life could be achieved by applying the endometriosis diet: a cross-sectional study in Dutch endometriosis patients. Reprod Biomed Online. 2023;46(3):623–630. https://doi.org/10.1016/j.rbmo.2022.12.010
-
Del Forno S, Cocchi L, Arena A, Pellizzone V, Lenzi J, Raffone A, et al. Effects of Pelvic Floor Muscle Physiotherapy on Urinary, Bowel, and Sexual Functions in Women with Deep Infiltrating Endometriosis: A Randomized Controlled Trial. Medicina (Kaunas). 2023;60(1):67. https://doi.org/10.3390/medicina60010067
-
Asociación Colombiana de Endometriosis e Infertilidad (ASOCOEN). Endometriosis Colombia. Consulta: Octubre 10, 2025. Disponible en: https://www.endometriosiscolombia.com/
-
Ministerio de Sanidad, Servicios Sociales e Igualdad. Guía de atención a las mujeres con endometriosis en el Sistema Nacional de Salud (SNS), 2013. Madrid (España). Consulta: Junio 26, 2025.
-
Krabbenborg I, de Roos N, van der Grinten P, Nap A. Diet quality and perceived effects of dietary changes in Dutch endometriosis patients: an observational study. Reprod Biomed Online. 2021;43(5):952–61. https://doi.org/10.1016/j.rbmo.2021.07.011
-
Liu P, Maharjan R, Wang Y, Zhang Y, Zhang Y, Xu C, et al. Association between dietary inflammatory index and risk of endometriosis: A population-based analysis. Frontiers in Nutrition. 2023;10:1077915. https://doi.org/10.3389/fnut.2023.1077915
-
Li X, Xie Z, Qiu H, Xie X, Liu L. Exploring the causal associations between diet-derived circulating antioxidants and the risk of endometriosis: a Mendelian randomization study. Frontiers in Nutrition. 2024;11:1453147. https://doi.org/10.3389/fnut.2024.1453147
-
Parasar P, Ozcan P, Terry KL. Endometriosis: Epidemiology, Diagnosis and Clinical Management. Curr Obstet Gynecol Rep. 2017;6(1):34-41. https://doi.org/10.1007/s13669-017-0187-1
-
Brouns F, Van Haaps A, Keszthelyi D, Venema K, Bongers M, Maas J, et al. Diet associations in endometriosis: a critical narrative assessment with special reference to gluten. Front Nutr. 2023;10:1295983. https://doi.org/10.3389/fnut.2023.1166929
-
Qin R, Tian G, Liu J, Cao L. The gut microbiota and endometriosis: From pathogenesis to diagnosis and treatment. Front Cell Infect Microbiol. 2022;12:1069557. https://doi.org/10.3389/fcimb.2022.1069557
-
Tennfjord MK, Gabrielsen R, Bø K, Engh ME, Molin M. Can general exercise training and pelvic floor muscle training be used as an empowering tool among women with endometriosis? Experiences among women with endometriosis participating in the intervention group of a randomized controlled trial. BMC Womens Health. 2024;24:505. https://doi.org/10.1186/s12905-024-03356-w
-
Sachs MK, Dedes I, El-Hadad S, Haufe A, Rueff D, Kohl Schwartz AS, et al. Physical Activity in Women with Endometriosis: Less or More Compared with a Healthy Control?. Int J Environ Res Public Health. 2023;20(17):6659. https://doi.org/10.3390/ijerph20176659
-
Tennfjord MK, Gabrielsen R, Tellum T. Effect of physical activity and exercise on endometriosis-associated symptoms: a systematic review. BMC Women's Health. 2021;21(1):355. https://doi.org/10.1186/s12905-021-01500-4
-
Martire FG, Costantini E, d’Abate C, Capria G, Piccione E, Andreoli A. Endometriosis and Nutrition: Therapeutic Perspectives. J. Clin. Med. 2025;14(11):3987. . https://doi.org/10.3390/jcm14113987
-
Thomas BH, Ciliska D, Dobbins M, Micucci S. A process for systematically reviewing the literature: providing the research evidence for public health nursing interventions. Worldviews Evid Based Nurs. 2004;1(3):176-84. https://doi.org/10.1111/j.1524-475X.2004.04006.x
-
Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. International Journal for Quality in Health Care. 2007;19(6):349–57. https://doi.org/10.1093/intqhc/mzm042
-
Fuentes Rodríguez A, Grela Beres O. Análisis de artículos del impacto de dieta y ejercicio físico en endometriosis. 2025. Mendeley Data: Versión 1. https://doi.org/10.17632/mky2ntyknm.1
-
Van Haaps AP, Wijbers JV, Schreurs AMF, Vlek S, Tuynman J, Bie BD, et al. The effect of dietary interventions on pain and quality of life in women diagnosed with endometriosis: a prospective study with control group. Hum Reprod. 2023;38(12):2433-2446. https://doi.org/10.1093/humrep/dead214
-
Eypasch E, Williams JI, Wood-Dauphinee S, Ure BM, Schmülling C, Neugebauer E, et al. Gastrointestinal Quality of Life Index: development, validation and application of a new instrument. British Journal Surgery 1995;82(2):216–22. https://doi.org/10.1002/bjs.1800820229
-
Looman M, Feskens EJ, Rijk M de, Meijboom S, Biesbroek S, Temme EH, et al. Development and evaluation of the Dutch Healthy Diet index 2015. Public Health Nutrition. 2017; 20(13):2289–99. https://doi.org/10.1017/S136898001700091X
-
Artacho-Cordón F, Salinas-Asensio MDM, Galiano-Castillo N, Ocón-Hernández O, Peinado FM, Mundo-López A, et al. Effect of a Multimodal Supervised Therapeutic Exercise Program on Quality of Life, Pain, and Lumbopelvic Impairments in Women With Endometriosis Unresponsive to Conventional Therapy: A Randomized Controlled Trial. Arch Phys Med Rehabil. 2023;104(11):1785–95. https://doi.org/10.1016/j.apmr.2023.06.020
-
Del Forno S, Arena A, Pellizzone V, Lenzi J, Raimondo D, Cocchi L, et al. Assessment of levator hiatal area using 3D/4D transperineal ultrasound in women with deep infiltrating endometriosis and superficial dyspareunia treated with pelvic floor muscle physiotherapy: randomized controlled trial. Ultrasound Obstet Gynecol. 2021;57(5):726–32. https://doi.org/10.1002/uog.23590
-
Nodler JL, Divasta AD, Vitonis AF, Karevicius S, Malsch M, Sarda V, et al. Supplementation with vitamin D or ω-3 fatty acids in adolescent girls and young women with endometriosis (SAGE): A double-blind, randomized, placebo-controlled trial. Am J Clin Nutr. 2020;112(1):229–36. https://doi.org/10.1093/ajcn/nqaa096
-
Barrea L, Verde L, Annunziata G, Chedraui P, Petraglia F, Cucalón G, et al. Effectiveness of Medical Nutrition Therapy in the Management of Patients with Obesity and Endometriosis: from the Mediterranean Diet To the Ketogenic Diet, Through Supplementation. The Role of the Nutritionist in Clinical Management. Curr Obes Rep. 2025;14:68. https://doi.org/10.1007/s13679-025-00662-8
-
Baradwan S, Gari A, Sabban H, Alshahrani MS, Khadawardi K, Bukhari IA, et al. The effect of antioxidant supplementation on dysmenorrhea and endometriosis-associated painful symptoms: a systematic review and meta-analysis of randomized clinical trials. Obstet Gynecol Sci. 2024;67(2):186-98. https://doi.org/10.5468/ogs.23210
-
Škegro B, Bjedov S, Mikuš M, Mustač F, Lešin J, Matijević V, et al. Endometriosis, Pain and Mental Health. Psychiatr Danub. 2021;3(l4):632–6. https://pubmed.ncbi.nlm.nih.gov/34718292/
-
Nap A, de Roos N. Endometriosis and the effects of dietary interventions: what are we looking for?. Reproduction and Fertility. 2022;3(2):C14–22. https://doi.org/10.1530/RAF-21-0110
-
Salinas-Asensio MdM, Ocón-Hernández O, Mundo-López A, Fernández-Lao C, Peinado FM, Padilla-Vinuesa C, et al. “Physio-EndEA” Study: A Randomized, Parallel-Group Controlled Trial to Evaluate the Effect of a Supervised and Adapted Therapeutic Exercise Program to Improve Quality of Life in Symptomatic Women Diagnosed with Endometriosis. Int J Environ Res Public Health. 2022;19(3):1738. https://doi.org/10.3390/ijerph19031738
-
Leroy R, Desimpel F, Ombelet S, De Jaeger M, Benahmed N, Camberlin C, et al. How can we improve endometriosis care in Belgium? KCE Report 378. Brussels (BE): Belgian Health Care Knowledge Centre (KCE); 2024. Consulta: octubre 10, 2025.
-
European Society of Human Reproduction and Embryology (ESHRE). ESHRE Guideline: Endometriosis. [Internet] Issued 2 February 2022 [Cited 16 June 2025] Disponible en: https://www.eshre.eu/guideline/endometriosis
-
Carvalho N, Margatho D, Cursino K, Benetti-Pinto CL, Bahamondes L. Control of endometriosis-associated pain with etonogestrel-releasing contraceptive implant and 52-mg levonorgestrel-releasing intrauterine system: randomized clinical trial. Fertil Steril. 2018;110(6):1129–36. https://doi.org/10.1016/j.fertnstert.2018.07.003
-
Harada T, Kobayashi T, Hirakawa A, Takayanagi T, Nogami M, Mochiyama T, et al. Efficacy and safety of the combination of estetrol 15 mg/drospirenone 3 mg in a cyclic regimen for the treatment of endometriosis-associated pain and objective gynecological findings: a multicenter, placebo-controlled, double-blind, randomized study. Fertil Steril. 2024;122(5):894–901. https://doi.org/10.1016/j.fertnstert.2024.07.011
-
Lee HJ, Yoon SH, Lee JH, Chung YJ, Park SY, Kim SW, et al. Clinical evaluation and management of endometriosis: 2024 guideline for Korean patients from the Korean Society of Endometriosis. Obstet Gynecol Sci. 2024;68(1):43-58. https://doi.org/10.5468/ogs.24242
-
National Institute for Health and Care Excellence (NICE). Endometriosis: diagnosis and management. NICE guideline [NG73]. London (UK): NICE; [Internet] 2017 [Cited 2025 Oct 8]. Available from: https://www.nice.org.uk/guidance/ng73/chapter/Recommendations#non-pharmacological-management